Open Access
Research Article
Max Screen
ISSN: 2639-9253
Copyright: © 2020 Subramanian A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Introduction: Microalbuminuria reflects rapid changes in glomerular permeability and is associated with systemic capillary permeability. This has been observed to predict outcome within few hours of insult in a wide variety of acute conditions including trauma. The objective of this three months duration study was to determine the levels of urinary microalbumin (MA) and correlate with outcomes in patients with traumatic brain injury (TBI) during Intensive care unit (ICU) stay
Material and Methods: Forty-three traumatic brain injury patients, admitted to our Level 1 trauma care centre ICU during three months study duration, were evaluated on three time points: within 24 hours of injury (day 1), day 3 and day 5 following ICU admission. On day 1, severity of head injury was evaluated using Glasgow Coma Scale (GCS). Microalbuminuria (MA) was defined as subclinical rise in the urinary albumin excretion within the range of 20mg/l to 200mg/l. Microalbuminuria (MA) levels were correlated with patients’ clinical outcome that included duration of ICU stay (<7, 7-14, >14 days), need for mechanical ventilation, sepsis and mortality.
Results: Out of 43 patients included in our study, 14 had moderate head injury (MHI; GCS 9-12) and 29 had severe head injury (SHI; GCS 3-8). Twenty five (58%) patients stayed in ICU for < 7 days, eight (19%) for 7-14 days and ten (23%) for >14 days; 34 (79%) required mechanical ventilation, 16 (37%) developed sepsis; none developed renal failure and 10 (23%) patients died. There is no influence of gender, blood pressure, mode of injury, severity of head injury (GCS) within 24 hours of injury on the MA levels. No correlation was found between sepsis, renal failure and need for mechanical ventilation. MA (20-200 mg/dl) was seen in 10%, 12% and 14% and mean MA levels were 8.3 mg/dl, 10.3 mg/dl and 14.3 mg/dl on day 1, day 3 and day 5 respectively. On admission raised MA levels correlated with prolonged ICU stay (>14days) (p=0.005).
Conclusion: Glomerular permeability was increased resulting in microalbuminuria in 26% of TBI patients in the ICU on admission and follow-up on day 3 and day 5. The study indicated that raised MA on admission can be utilized to predict longer ICU stay in TBI patients which is simple noninvasive and inexpensive bedside tool.
Keywords: Microalbuminuria; Glomerular Permeability; Traumatic Brain Injury
Trauma induces a systemic inflammatory response that activates humoral and cellular inflammatory mediators and releases wellknown cytokines [1,2] resulting in increase in capillary permeability that occurs within minutes of injury [3]. Generalised systemic vascular permeability can also be reflected by glomerular permeability. Various methods have been proposed to determine the capillary permeability like radiolabelled albumin method [4] indicator diffusion method [5] and thermal green dye indicator dilution method [6]. But all these techniques are time consuming and expensive. Microalbumin has also been found to be an important marker of glomerular permeability and hence systemic vascular permeability. Since it is important prognostic indicator in trauma [3], surgery [3], ischemia reperfusion injury [3], acute pancreatitis [3], meningitis [3], malignancies, hypertension and predictor of organ failure and mortality in ICU patients [7-9], we evaluated its role in TBI. In our study only TBI patients are included as opposed to mixed ICU (medical and surgical) patients in the previous studies. As medical conditions like diabetes and hypertension are independent causes of microalbuminuria, excluding them might have added relevance to the present study.
Microalbuminuria (MA) is defined as sub-clinical rise in the urinary albumin excretion. Hasslacher et al. defined MA as albumin excretion in the urine within the range of 20mg/l to 200mg/l [10]. Prevalence of microalbuminuria in normal healthy adults is up to 3.3% [11]. The degree of microalbuminuria can also be indexed with a spot urine albumin-creatinine ratio (ACR) [12].
The objective of this longitudinal study was to determine the levels of urinary microalbumin (MA) in patients with traumatic brain injury (TBI) during ICU admission and correlate with patients’ four clinical outcomes that included mortality, sepsis, requirement of mechanical ventilation and duration of ICU stay (< 7, 7-14, >14 days).
In this longitudinal study, 43 trauma patients with head injury admitted to the ICU at Jai Prakash Narayan Apex Trauma Centre, AIIMS between age group 16-65 years during the study period of three months were evaluated. Patients with anuria, overtly bloody urine, on renal replacement therapy, existing chronic renal disease (serum creatinine level ≥ 2 mg dl), diagnosis of type 1 or type 2 diabetes mellitus and receiving nephrotoxic drugs were excluded from the study
On the day of admission (day 1) severity of head injury was calculated using Glasgow coma Scale. Urine microalbumin was measured at three time points; day 1, day 3 and day 5 of admission in the ICU. Other parameters like time elapsed from injury to admission, length of stay in ICU, mode of injury and hypotension (systolic blood pressure < 90mm/hg) were also noted. All these parameters were correlated with patients’ four clinical outcomes that included mortality, sepsis (SIRS and culture positive), requirement of mechanical ventilation and duration of ICU stay (< 7, 7-14, >14 days).
All parameters were measured on Beckman Coulter Unicel dxc800. MA reagent was used in conjunction with unicel® dxc 600/800 system(s) and synchron® systems MA calibrator for automated quantitative determination of albumin concentration in human urine. Urine samples were collected without a preservative. Turbidity if any or particulate matter was clarified by centrifugation (3000 x g for 10 minutes). Urine albumin was measured by automated turbidimetry using MA antibody specific for human albumin (goat). Results were expressed as the MA levels in mg/l. Microalbuminuria (MA) is defined as sub-clinical rise in the urinary albumin excretion in the range of 20-200 mg/l in a spot urine examination [10].
It was done using Mann-Whitney Ranksum test, Bonferroni’s test, paired t test and chi- square test (Figure 1).
Overall mean age was 35±14 years and median time elapsed from injury to admission in ICU was 6.5 (1-48) hrs. Most common mode of head injury was road traffic accident (70%). Males outnumbered females (M: F=6:1). Three patients had hypotension. Out of 43 patients, 14 patients had moderate head injury (MHI; GCS 9-12) and 29 had severe head injury (SHI; GCS 3-8) (Table 1).
Microalbuminuria on day 1, day 3 and day 5 was seen in 10%, 12% and 14% respectively (Figure 2) and mean MA levels were rising steadily on day 1, day 3 and day 5 which were 8.3, 10.3 and 14.3 mg/dl respectively (Figure 3).
Out of 43 patients, 14 had moderate head injury (GCS 9-12) and 29 had severe head injury (GCS 3-8) (Table 1). Twenty five (58%) patients stayed in ICU for < 7 days, 08(19%) for 7-14 days and 10(23%) for >14 days; 34 (79%) required mechanical ventilation, 16(37%) developed sepsis; and 10 (23%) patients died (Table 2).
All patients had normal values of blood urea and serum creatinine and no one developed renal failure.
29% of moderate head injury patients and 24% of severe head injury patients had microalbuminuria during the course of stay in ICU. Microalbumin levels in moderate head injury patients increased from day 1 to day 5 and in severe head injury patients increased from day 1 to day 3 and again decreased on day 5 although results were not significant (Table 3).
There was no influence of sex, blood pressure, mode of injury and GCS (Glasgow Coma Scale) within 24 hours of injury on the microalbumin levels.
ICU stay:Twenty five (58%) patients stayed in ICU for < 7 days, 08 (19%) for 7-14 days and 10 (23%) patients for >14 days. Patients with longer ICU stay (>7 days) had significantly raised microalbumin levels (p=0.02; p=0.005, < 7 days vs. 7-14 days) on day 1. No correlation with mechanical ventilation, sex, blood pressure and GCS was found.
Mechanical ventilation: Out of 43 patients, 34(79%) required mechanical ventilation. There was no significant difference in the blood pressure, duration of stay in ICU and GCS at the time of admission between the two groups. No significant difference in microalbumin levels in patients requiring and not requiring mechanical ventilation was seen.
Sepsis:16 out of 43 patients developed sepsis later in their disease course. There was no significant difference in the blood pressure, duration of stay in ICU and GCS at the time of admission. Microalbumin levels in patients remained almost same irrespective of the development of sepsis.
Mortality:Out of 43 patients, 10 (23%) died. Median age of patients who died was 32 yrs and all were males. There was no significant difference between survivors and non survivors in the blood pressure and GCS at the time of admission. Cause of death in 50% of the patients was cardiac arrest. However, day 5 microalbumin levels decreased significantly in patients who died (p=0.02), so decreased values of MA on day 5 can be correlated with increased risk of mortality (Table 4).
The reason for increased incidence of microalbuminuria in critically ill patients as compared with general population is probably due to widespread endothelial dysfunction arising from the effects of cytokines, and other inflammatory mediators, released during the intense inflammatory responses that are associated with critical illnesses [13]. The effects of disruption of the integrity of the endothelial barrier is manifested as altered glomerular endothelial permeability in the kidneys, allowing increased amounts of albumin to escape into the glomerular ultrafiltrate. The tubular reabsorptive mechanism for albumin from the ultrafiltrate is exceeded beyond its threshold capacity, leading to increased excretion of albumin in the urine. The degree of albuminuria is dependent on the intensity of the inflammatory responses, and therefore microalbuminuria reflects disease severity. 11. Recognition of Anesthesia as an Independent Speciality
In present study, microalbuminuria was seen in 26% of the patients and mean MA levels were rising steadily from day 1 to day 3 and day 5. Various studies showed transient microalbuminuria in 70% (8), 71% [13], 76% and 90% ICU patients which is higher as compared to our study. Few studies also reported higher incidence of microalbuminuria in medical patients in comparison to surgical patients [14,15]. In our study only head injury patients are included as opposed to heterogeneous groups of mixed medical and surgical patients in previous studies. As medical conditions like diabetes and hypertension are independent causes of microalbuminuria, excluding them might have added relevance to the present study
Microalbumin levels in moderate head injury increased from day 1 to day 5 and in severe head injury patients increased from day 1 to day 3 and again decreased on day 5 although results were not significant. Patients with longer ICU stay (>7 days) had significantly raised microalbumin levels (p=0.02; p=0.005, < 7 days vs. 7-14 days) on day 1. The patients who stayed longer than 14 days had raised MA levels on day 1.
Gaudio et al. [2] studied 40 critically ill trauma patients and observed an increase in glomerular permeability during the first 24 h after trauma however it did not have a positive predictive value with respect to severity of illness (ISS).
Mackinnon et al [9] studied 50 mixed ICU patients at 6 hrs after admission and significant difference between survivors and non survivors was seen allowing earlier and rapid identification of patients at increased risk of developing organ failure and increased risk of death. However, MA levels on day 5 decreased significantly in non-survivors (p=0.02).
In this context, the work of Abid et al. [16] on the prognostic value of microalbuminuria is significant. They measured MA at 8 h after hospital admission and repeated this measurement for 5 days and followed changes in microalbuminuria with time. They found that patients with increasing microalbuminuria, suggesting progressive inflammation, had a worse outcome and higher mortality than those who had a decreasing trend.
Gosling et al. [15] studied ACR within first 6 hours on 431 patients in mixed medical and surgical ICU and reported that it significantly correlated with duration of mechanical ventilation, length of ICU stay, and ICU mortality. Yew et al [11] also observed significant correlation between ACR and mortality.
Zhang et al [17] concluded that microalbuminuria measured on entry to ICU is predictive of the development of acute renal injury in septic patients, higher urinary albumin to creatinine ratio (ACR) was associated with higher mortality and longer ICU length of stay and the use of microalbuminuria (>143 mg/g) can help identify patients at high risk of acute renal injury
Croal et al. [18] observed that the average length of stay in patients with normal ACR was significantly less than for those patients with an abnormal ACR thus concluding that microalbuminuria status can be used as a potential immediate risk management tool in intensive care.
Dutta et al. [19] concluded that microalbuminuria has a good diagnostic and prognostic significance in sepsis as compared to APACHE score and Tnf-α
Patel et al. [13] found that non-survivors had higher levels of microalbuminuria on ICU admission compared to survivors. Also there was significant increase in microalbuminuria in nonsurvivors at 24 hrs.
Basu et al. [14] studied 525 mixed medical and surgical ICU patients and concluded that microalbuminuria was raised in 76% of patients measured as ACR at 24 hrs of ICU admission is as good a predictor of mortality as the APACHE score in critically ill patients. They observed direct correlation between MA levels and duration of ICU stay.
In our study out of 43 patients, 34 (79%) required mechanical ventilation. No significant difference in microalbumin levels in patients requiring and not requiring mechanical ventilation was seen. However, Basu et al [14] observed significant correlation between microalbuminuria and duration of mechanical ventilation. Honarmand et al in 2009 [8] concluded that the albumin- creatinine ratio can be used in estimating the risk of prolonged mechanical ventilation, even on the first day of admission of critically ill trauma patients. Similar results were obtained by Sorour et al. [1] in 2015 who concluded that albumin-creatinine ratio on admission and at 24 hours predicted duration of mechanical ventilation.
In our study, 16 out of 43 patients developed sepsis later in the course of ICU stay. There was no significant difference in the blood pressure; time elapsed from injury to admission, duration of stay in ICU and GCS between the two groups. Microalbumin levels in patients remained almost same irrespective of the development of sepsis. Tayeh et al. [20] evaluated the prognostic value of albumin-creatinine ratio in patients with sepsis and concluded that ACR may be used as a simple test for prognosis and mortality prediction in sepsis. Szakmany et al [21] studied critically ill patients in ICU and concluded that MA: CR measured on admission to the ICU was significantly higher in non-survivors than in survivors. Godijn N et al. [22] also concluded that ACR increases in the first five days in all critically ill patients, however no statistical significant difference was found between survivors and non survivors. Gagarin PY et al. [23] revealed that microalbuminuria was weakly correlated with the mortality of the ICU patients. Therefore, further studies could be directed towards evaluating the use of microalbuminuria in monitoring the efficacy of individual therapeutic interventions which impact survival in critically ill patients.
Glomerular permeability was increased due to trauma resulting in transient microalbuminuria in 26% of patients in ICU on admission and on follow-up on day 3 and day 5. Also, on admission elevation of microalbuminuria correlated with longer ICU stay. Based on these results, we conclude that TBI can trigger an increase above normal in glomerular permeability and can predict longer ICU stay in TBI patients however this increase is not related to severity of illness and/or outcome in ICU in terms of requirement of mechanical ventilation, sepsis and mortality. We recommend a further study on a larger cohort to analyse the clinical significance of our findings.

![]()

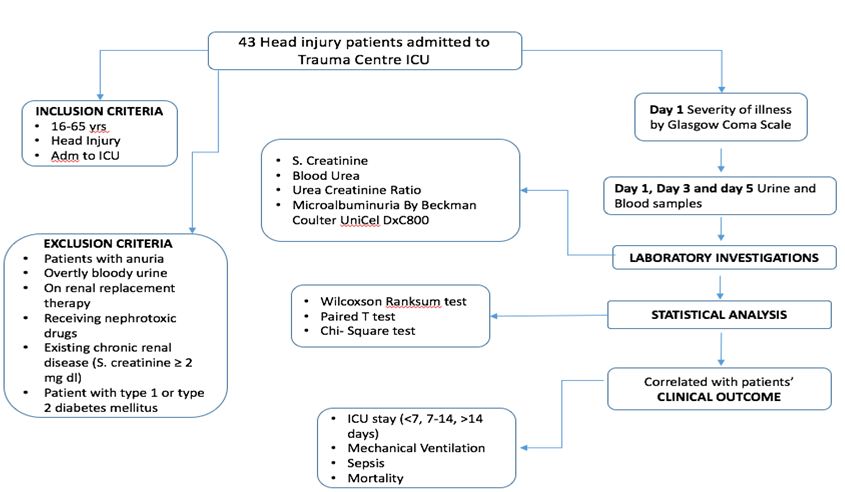 |
| Figure 1: Methodology |
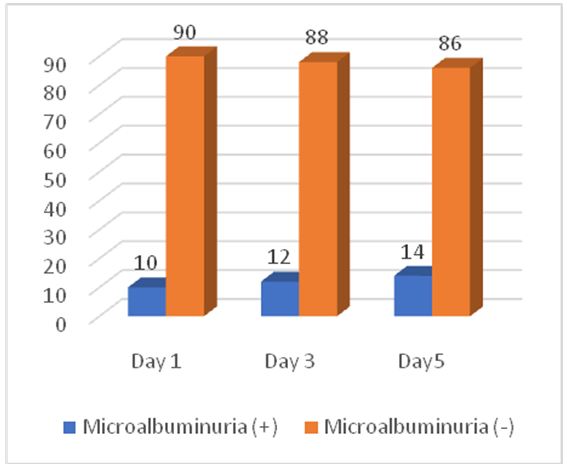 |
| Figure 2: Percentage of Patients having Microalbuminuria on day 1, 3 and 5. |
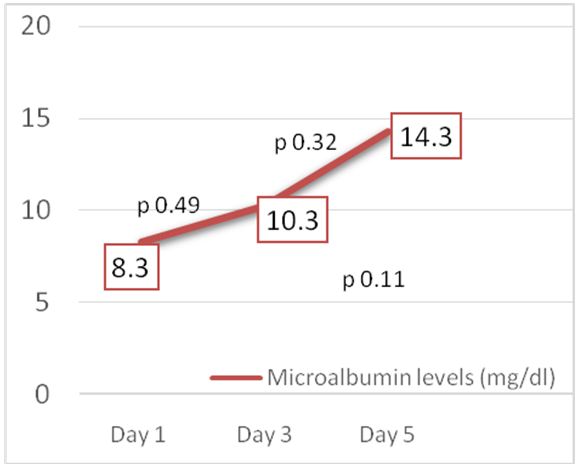 |
| Figure 3: Microalbuminuria levels (mg/dl) on day 1, 3 and 5. |
General Demographics |
Number (%) |
|
Age |
35(17-65) years |
|
Gender |
Male |
37(86) |
Female |
6(14) |
|
Mode of injury |
RTA |
30(70) |
Fall |
9(22) |
|
Assault |
4(10) |
|
Time elapsed from injury to admission (hrs) |
≤6 |
20(50) |
7-12 |
12(30) |
|
12-24 |
6(15) |
|
≥24 |
2(5) |
|
Hypotension (systolic blood pressure <90mm/hg) |
Yes |
3(7) |
No |
39(93) |
|
Severity of head injury |
Severe (GCS 3-8) (SHI) |
29(67) |
Moderate(GCS 9-12) (MHI) |
14(33) |
|
Parameter |
Number (%) |
|
Mechanical ventilation |
Yes |
34(79) |
No |
9(21) |
|
Sepsis |
Yes |
16(37) |
No |
27(63) |
|
ICU stay (days) |
<7 |
25(58) |
7-14 |
8(19) |
|
>14 |
10(23) |
|
Mortality |
Yes |
10(23) |
No |
33(77) |
|
Head Injury |
Microalbuminuria ; median (interquartile range) |
P value |
|||
Day 1 |
Day 3 |
Day 5 |
|||
Moderate (GCS 9-12) |
3.0(1.8-10.9) |
3.0(2.9-2.1) |
3.4(3.3-2.0) |
Day 1 vs 3 |
0.5709 |
Day 1 vs 5 |
0.3771 |
||||
Day 3 vs 5 |
0.9532 |
||||
Severe |
2.3(1.2-5.6) |
4.0(3.6-1.4) |
2.3(2.-1.1) |
Day 1 vs 3 |
0.72 |
Day 1 vs 5 |
0.17 |
||||
Day 3 vs 5 |
0.23 |
||||
P value |
0.90 |
0.67 |
0.63 |
|
|
Outcomes (No. Of patients) |
Microalbuminuria (mean ± SD) |
P value |
||||
Day 1 |
Day 3 |
Day 5 |
||||
ICU (days) |
<7 (25/43) |
2.7(0.6-33.1) |
3.6(0.3-88) |
3.8(0.4-117) |
Day 1 vs 3 |
0.67 |
Day 1 vs 5 |
0.08 |
|||||
Day 3 vs 5 |
0.21 |
|||||
7-14 (8/43) |
1.25(0.4-6.8) |
2.1(0.5-6.5) |
2.3(1.1-7.5) |
Day 1 vs 3 |
0.54 |
|
Day 1 vs 5 |
0.35 |
|||||
Day 3 vs 5 |
0.80 |
|||||
>14 (10/43) |
2.75(0.9-75) |
8.05(0.6-70) |
4.3(1-69) |
Day 1 vs 3 |
0.62 |
|
Day 1 vs 5 |
0.90 |
|||||
Day 3 vs 5 |
0.32 |
|||||
|
P - value |
0.02 |
0.07 |
0.81 |
|
|
Post hoc;1 vs 2= 0.005, 1 vs 3= 0.79 and 2 vs 3= 0.06 |
|
|||||
Mechanical ventilation |
Required |
8.2±2.6 |
10.7±3.4 |
14.6±4.7 |
Day 1 vs 3 |
0.45 |
Day 1 vs 5 |
0.15 |
|||||
Day 3 vs 5 |
0.42 |
|||||
Not required |
9.2±3.9 |
8.7±3.3 |
13.0±5.4 |
Day 1 vs 3 |
0.92 |
|
Day 1 vs 5 |
0.52 |
|||||
Day 3 vs 5
|
0.46 |
|||||
P - value |
0.85 |
0.78 |
0.86 |
|
|
|
Sepsis |
Yes (16/43) |
10.6±5.1 |
12.1±4.6 |
10.8±5.2 |
Day 1 vs 3 |
0.69 |
Day 1 vs 5 |
0.97 |
|||||
Day 3 vs 5 |
0.71 |
|||||
No (27/43) |
7.0±1.8 |
9.2±3.4 |
16.4±5.4 |
Day 1 vs 3 |
0.58 |
|
Day 1 vs 5 |
0.08 |
|||||
Day 3 vs 5 |
0.24 |
|||||
P - value |
0.44 |
0.61 |
0.49 |
|
|
|
Mortality |
Dead (10/43) |
2.6(0.8-20.1) |
2.6(0.6-12.3) |
1.1(1-13.3) |
Day 1 vs 3 |
0.51 |
Day 1 vs 5 |
0.07 |
|||||
Day 3 vs 5 |
0.61 |
|||||
Alive (33/43) |
2.3(0.4-75) |
5(0.3-88) |
4.1(0.4-117) |
Day 1 vs 3 |
0.40 |
|
Day 1 vs 5 |
0.07 |
|||||
Day 3 vs 5 |
0.29 |
|||||
|
P - value |
0.8 |
0.38 |
0.02 |
|
|




































