Open Access
Research Article
Max Screen
ISSN: 2770-839X
Copyright: © 2022 Arenas Soto CM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Atopic dermatitis is a common chronic disease in children. One of its possible exacerbating factors is covid-19 infection. We present the case of a patient with exacerbation of his atopic dermatitis due to COVID-19 infection.
Keywords: Atopic Dermatitis; Covid-19; Exacerbation
List of abbreviations:Covid-19: Coronavirus Disease 2019; SARS-CoV-2: The Severe Acute Respiratory Syndrome Coronavirus 2; AD: Atopic Dermatitis; RT-PCR: Reverse Transcription - Polymerase Chain Reaction
The coronavirus disease 2019 (COVID-19) is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1]. This infection has registered millions of cases and deaths worldwide for which it is considered a threat to public health [2]. This infection can induce changes in people's living conditions, with important consequences for general health and on coexisting diseases, such as atopic dermatitis (AD), rosacea and psoriasis [1,3].
AD is a multifactorial entity that affects the skin, where intrinsic and extrinsic factors interact to be the cause and consequence of the exacerbation of the disease; in times of pandemic, emotional stress triggered by strict home confinement, fear of contracting coronavirus infection, frequent hand washing and sanitizing are factors that are mainly related [1,3]. Also, the dysregulation of the immune system in chronic inflammatory dermatological diseases are associated with an increase in cytokines and inflammatory mediators, like Covid-19, with a predominance of the Th1 pathway (IL 6, IL 2 and TNF-α) [1,3]; the cytokines of the Th2 pathway have little been studied with the infection by SARS-CoV-2 [4].
We present the case of a patient with an exacerbation of his atopic dermatitis due to COVID-19 infection, stress and preventive hygiene measures.
An 11-year-old boy, student, with a history of atopic dermatitis diagnosed at 11 months of age without referring to another significant history (Figure 1), undergoing treatment only with soap substitutes and topical corticosteroids in periods of exacerbation of the disease. The last exacerbation of him reported by the mother 5 months ago.
During the period of strict home confinement, he presented SARS-CoV-2 COVID-19 infection confirmed by RT-PCR from nasopharyngeal swab, characterized by 4 days of evolution of headache, dry cough, fever, asthenia, adynamia, without requiring Hospital admission, associated with burning, intense itching and skin lesions on bleeding fingers, antecubital folds, neck and abdomen.
On physical examination, erythematous, scaly, fissured plaques were observed on the pads of the fingers (Figure 2A), erythematous, edematous, scaly plaques on the back of the hands (Figure 2B), neck, abdomen and antecubital folds (Figure 2C). In the clinimetric evaluation, he presented an EASI: 1.6 POEM: 15 HADS: 5.
He referred as preventive measures to reduce the risk of coronavirus infection washing hands with soap substitutes more than 10 times a day, disinfecting hands more than 10 times a day, did not use moisturizers and bathed with water hot. The previous preventive measures were taken by the minor because his father had a SARS CoV2- COVID 19 infection.
He presents a diagnosis of SARS CoV-2 infection and exacerbation of mild-moderate AD. He received symptomatic treatment for the coronavirus infection with acetaminophen and an antihistamine. He didn’t require antiviral treatments. In addition, he was treated for his atopic dermatitis with soap substitute, moisturizer and betamethasone dipropionate 0.05% once a day for 20 days with resolution of his symptoms.
AD is a chronic inflammatory disease of the skin with a prevalence of 20% in children and 2-10% in adults [5]
It is a heterogeneous and multifactorial entity with a complex pathophysiology, where intrinsic and extrinsic factors interact such as age, sex, genetics, integrity of the skin barrier and the Western lifestyle, pollution, stress and atmospheric elements, respectively [6]. These factors can affect the prevalence and severity of the disease and result in skin barrier dysfunction, transpidermal water loss, and dysregulation of the immune system [6-8].
The association between AD and COVID-19 is poorly understood, where AD patients do not have a greater predisposition to a more severe course of coronavirus infection [6]. In a retrospective analysis of 21 AD patients who presented Covid-19, it was found that 3 of 7 patients with mild infection had a mild worsening of their AD. Furthermore, these patients had no differences in length of hospital stay, treatment, or prognosis compared to Covid-19 patients without AD [5].
It should be taken into account that measures to minimize the risk of coronavirus infection, such as the prolonged use of personal protective equipment, disinfection and repeated hand washing (more than 10 times a day), can induce a alteration of the skin barrier and increase exposure to irritants agents [9,10]. This cause a subsequent eczema on the hands and face [5,6,11,12], as observed in our case and as has been reported in several publications [13]. In addition, the intensive use of soap, hot water and the sanitization of surfaces is related with exacerbation of AD [13].
On the other hand, AD patients may have experienced an exacerbation of the disease due to the lifestyle in quarantine during the COVID-19 pandemic, including home confinement and increased psychological effects such as chronic stress that can increase itching in some chronic skin diseases, also due to neuroendocrine modulation of skin inflammation [6,13]. Also, it must be taken into account that the drugs used for the treatment of COVID-19, especially intravenous corticosteroids, can cause a rebound effect in the symptoms of atopic dermatitis [13].
In conclusion, more studies are needed to clarify the relationship between the immune system and SARS CoV-2 COVID-19 infection, specifically with AD. Also, emotional stress during the pandemic triggered by strict home confinement, fear of contracting coronavirus infection, frequent hand washing and sanitizing (more than 10 times a day), are factors that are related to the exacerbation of AD and predispose to exposure to irritants.
These measures must be maintained to minimize the risk of coronavirus infection. But in patients with AD, some strategies are implemented such as: hand washing with warm water, mild hand cleanser, application of moisturizing hand creams, and others. Additionally, all patients should be recommended to continue with the treatments to control their underlying disease, to date they do not indicate an increased risk of SARS-CoV-2 infection.
The authors declare that they have no conflicts of interest. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Written informed consent was obtained from the patient for his anonymized information to be published in this article.

![]()

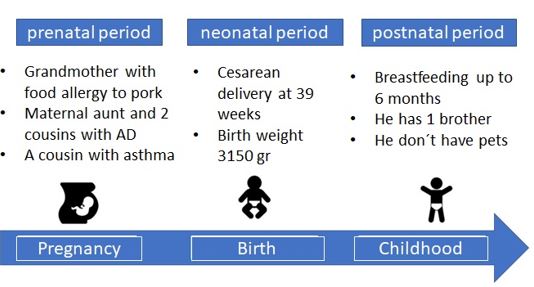 |
| Figure 1: Antecedents in the prenatal, neonatal and postnatal period |
 |
| Figure 2: (A) Erythematous plaques with cracks in fingertips; (B) Numerous erythematous, edematous and scaly plaques are present on the hands; (C) Also, erythematous and scaly plaques in abdomen and antecubital folds |




































