Open Access
Research Article
Max Screen
ISSN: 2770-839X
Copyright: © 2021 Kim Y. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Melanoma is one of the most fatal disorders dermatologists have to diagnose and treat. Despite its prevalence and seriousness, there has been no protocol with consensus suggesting systematic approach for diagnosis and treatment of pigmented lesions. A series of 141 melanomas diagnosed and managed over five years in an Australian dermatology clinic are presented. Also a systematic approach has been suggested for the management of suspicious pigmented lesions and melanomas. It is hoped that this paper provides a platform to open discussion for the development of the best systematic approach.
Keywords: Melanoma; Shave Excision; Mapping Biopsy; Aussie Kim approach
Melanoma is one of the most fatal disorders dermatologists have to diagnose and treat [1]. Even though many dermatologists are managing suspicious pigmented lesions and melanomas on a day to day basis, there has been no single agreed approach to a suspicious pigmented lesion. A series of 141 melanomas diagnosed and managed over five years in an Australian dermatology clinic are presented. In addition, an approach has been suggested to manage suspicious pigmented lesions.
Melanomas diagnosed and managed in an Australian dermatology private practice by one dermatologist between 2016 and 2020 are included. This private practice operated for 32 hours per week for patient appointments throughout this period. All the wider excisions were performed in the same clinic. Melanomas diagnosed at a separate teaching facility and referred for wide excision were excluded (approximately an extra three to five cases a year). In addition, severely dysplastic naevi were excluded (approximately 10 cases per year). Patients with lesions diagnosed by doctors at other clinics and referred for wide excisions were excluded as well.
All suspicious lesions were initially managed by shave excision. Shave excision should not be confused with shave biopsy. The intention of shave excision is to achieve margin clearance, not partial biopsy. Disposable biopsy blades (Kai medical, Japan) were used for lesions upon the limbs and trunk, whilst 15c blades were utilised upon facial lesions (Figure 1). When melanoma was diagnosed and shave margins were clear, wider excision was performed. If shave margins were involved, orientated mapping shave biopsies were performed to ascertain the extent and exact location of the residual melanoma (Figure 2), then wider excision was performed. All the patients whose lesions had a Breslow thickness greater than 1 mm underwent PET scan to exclude metastasis.
Patients with Clark level 1 melanoma were followed up every 6 months for the first 5 years, then yearly, whereas patients with Clark level 2 and above were followed up every 3 to 4 months for the first 2 years followed by 6 monthly for the following 3 years, then yearly. Patients who had PET scan had repeat PET scan at 12 months follow up (Figure 3).
A total of 141 melanomas were diagnosed and managed during this period (Table 1). There were four patients with two melanomas, as well as one patient with three melanomas diagnosed simultaneously. The mean age of the patients was 66.1 years, with those in their 20’s accounting for 2.8% (n=4), 30’s 1.4% (n=2), 40’s 12.8% (n=18), 50’s 14.9%, (n=21), 60’s 25.5% (n=36), 70’s 22.0% (n=31), 80’s 14.9% (n=21), and 90’s 5.7% (n=8). Almost 70% of patients were older than 60 years.
Clark level 1 accounted for 69.5% of melanoma (n=98), with level 2 16.3% (n=23), level 3 7.1% (n=10), level 4 6.4% (n=9), and level 5 0.7% (n=1). By location, the face was the most common site, accounting for 24.8% (n=35), followed by back 18.4% (n=26), both arms and legs 12.8% each (n=18 for each), neck 7.8% (n=11), shoulder 6.4% (n=9), abdomen 5.7% (n=8), chest 3.5% (n=5), both scalp and ears 2.8% each (n=4 for each), and buttock 1.4% (n=2).
Superficial spreading melanoma was the most common subtype (Table 2), accounting for 51.1% (n=72), followed by lentigo maligna 39.7.4% (n=56), combined superficial spreading and lentigo maligna 3.5% (n=5), nodular 2.8% (n=4), amelanotic 1.4% (n=2), naevoid 0.7% (n=1), desmoplastic 0.7% (n=1).
Of the 141 melanomas diagnosed, 29.8% had mapping biopsies performed (n=43), with two cases requiring mapping biopsy twice for margin clearance. None of the cases had margin involvement on wide excision.
It would be beneficial to all dermatologists if a practical and efficient protocol was developed to manage suspicious pigmented lesions. The dermatology clinic where the cases were diagnosed also has a surgical interest, and so was fortunate enough to be able to manage the melanomas from initial diagnosis to wider excision, and will subsequently be able to provide long term follow up.
The approach used in this series has two distinct points: shave excision and mapping biopsy.
The intention of shave excision is to achieve margin clearance, not partial biopsy. Some dermatologists advocate for excisional biopsy with various margins. If excisional biopsy is performed and confirms melanoma, further excision is often required depending on the Clark level and Breslow thickness of the melanoma. Also, if the histology shows mildly or moderately dysplastic naevus, shave excision would have been sufficient without further excision [2,3]. Shave excision is a much more time efficient and economical way to achieve a diagnosis, and prevents multiple excisions in the case of melanoma.
Mapping biopsies can prevent multiple excisions to achieve margin clearance, particularly in case of lentigo maligna, where margins can be very difficult to assess clinically. Mapping biopsies are similar to slow Mohs surgery; however the histology is assessed by a pathologist so it can be performed by any non-Mohs dermatologist. In addition immunohistochemistry/deeper levels may be performed to assess accurate margins if required, as further mapping biopsies or wider excision can be delayed for few days.
In this series, all cases were given options of sentinel lymph node biopsy prior to the wider excision, but all patients declined when it was explained that there was no proven survival advantage [4,5]. Positive sentinel lymph node biopsy may qualify for preventive immunotherapy in some countries, but this discussion is beyond the scope of this paper. In addition, further studies to establish any survival difference between patients investigated with PET scan and sentinel lymph node biopsy would be helpful.
The case numbers in this study are too small to provide meaningful epidemiological data. However, these numbers should be sufficient to support the functionality of the systematic approach the author suggests. The author suggests the name “Aussie Kim approach” for the management of a suspicious pigmented lesion described in this paper.
The author would like thank Ms Kristy Kim RN and Dr Louis Pool FRCPA and Dr Fiona Lehane FRCPA for their great input into this paper.
This article has no funding source.
The author has no conflict of interest to declare. This content has never been presented previously

![]()

 |
| Figure 1: Disposable biopsy blade (Kai medical, Japan) and 15c blade used for shave excision |
 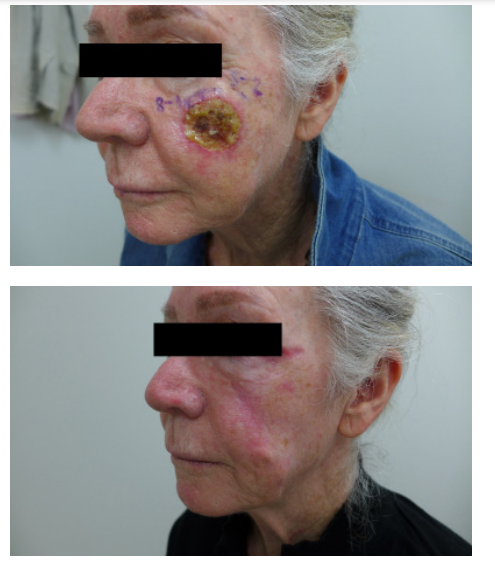 |
| Figure 2: Initial shave excision, 2 mapping biopsies to achieve margin clearance, and 6 months after wider excision of level 2 lentigo maligna melanoma |
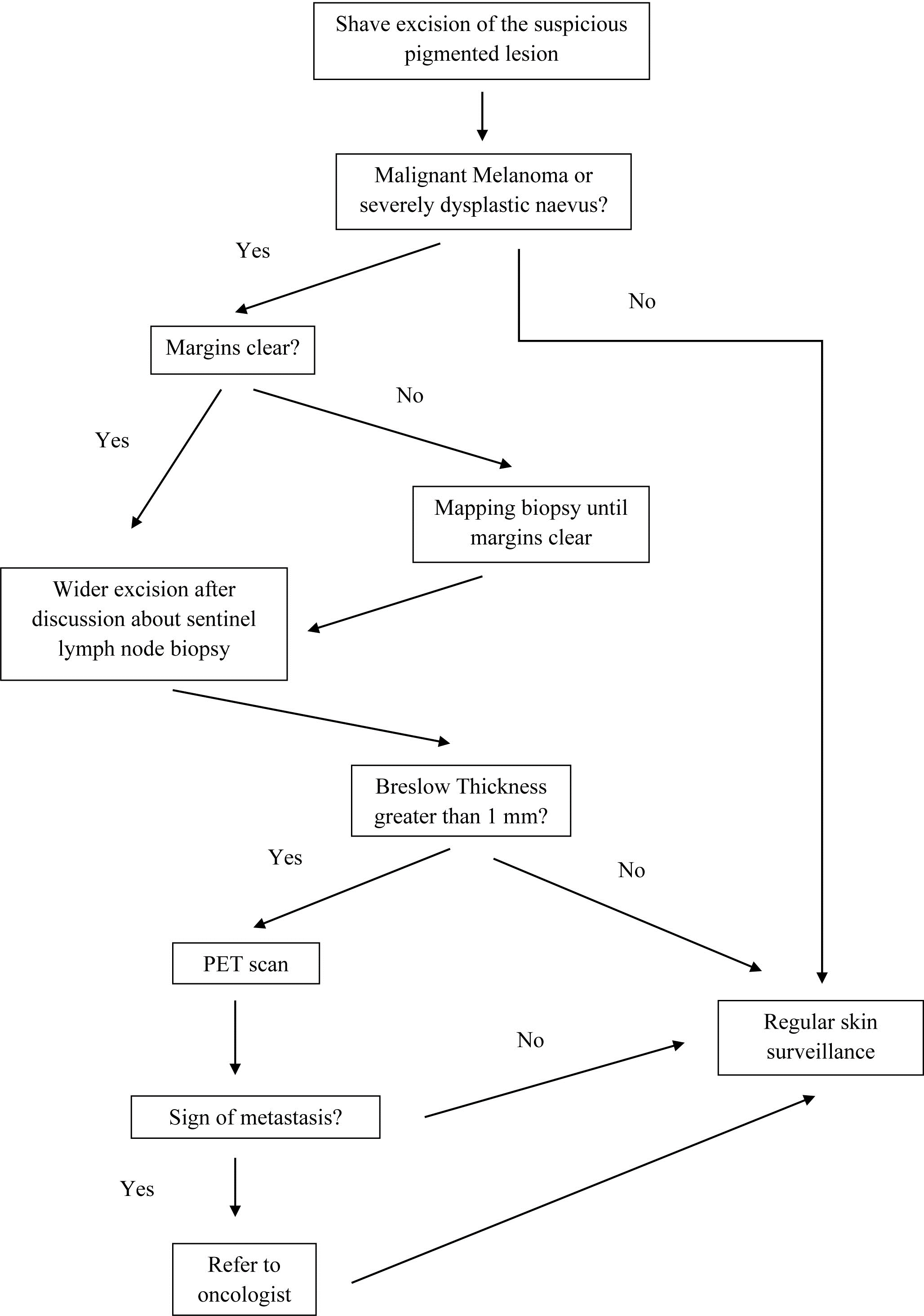 |
| Figure 3: "Aussie Kim approach" for the suspicious pigmented lesion |
Year |
Age |
Site |
Type |
Clark |
Breslaw |
Mapping |
2016 |
66 |
Right Lateral |
Lentigo Maligna |
1 |
|
No |
|
66 |
Left Anterior Thigh |
Superficial Spreading |
2 |
0.5 |
No |
|
60 |
Mid Chest |
Superficial Spreading |
2 |
0.6 |
No |
|
47 |
Right Posterior Calf |
Superficial Spreading |
1 |
|
No |
|
53 |
Right Deltoid |
Superficial Spreading |
1 |
|
No |
|
58 |
Left Buttock |
Superficial Spreading |
3 |
0.8 |
No |
|
83 |
Right Posterior |
Superficial Spreading |
1 |
|
No |
|
61 |
Left Posterior Ear |
Superficial Spreading |
2 |
0.3 |
No |
|
56 |
Left Cheek |
Lentigo Maligna |
1 |
|
No |
|
48 |
Right Mid Back |
Superficial Spreading |
1 |
|
No |
|
48 |
Right Posterior Calf |
Superficial Spreading |
1 |
|
No |
|
31 |
Left Base Of The |
Amelanotic Nodular |
3 |
1.0 |
No |
|
22 |
Right Lateral Neck |
Superficial Spreading |
2 |
0.4 |
No |
|
55 |
Right Lateral Thigh |
Superficial Spreading |
2 |
0.3 |
No |
|
68 |
Right Posterior Thigh |
Superficial Spreading |
1 |
|
No |
|
85 |
Left Upper Back |
Superficial Spreading |
1 |
|
No |
|
29 |
Left Posterior Calf |
Superficial Spreading |
1 |
|
No |
|
76 |
Left Mid Back |
Superficial Spreading |
1 |
|
No |
|
76 |
Right Earlobe Mid |
Superficial Spreading |
2 |
0.4 |
Yes |
|
64 |
Mid Glabella |
Amelanotic Nodular |
3 |
1.0 |
No |
|
70 |
Left Lower Cheek |
Lentigo Maligna |
1 |
|
No |
|
66 |
Right Cheek |
Lentigo Maligna |
1 |
|
Yes |
|
93 |
Left Anterior Shin |
Superficial Spreading |
2 |
0.3 |
No |
|
58 |
Left Anterior Shin |
Superficial Spreading |
4 |
1.5 |
No |
|
95 |
Right Cheek |
Lentigo Maligna |
1 |
|
Yes |
|
44 |
Right Abdo |
Lentigo Maligna |
1 |
|
No |
|
77 |
Left Upper Back |
Superficial Spreading |
1 |
|
No |
|
82 |
Left Temple |
Lentigo Maligna |
1 |
|
Yes |
|
48 |
Left Anterior Thigh |
Superficial Spreading |
1 |
|
No |
|
69 |
Right Lateral Shin |
Superficial Spreading |
1 |
|
No |
2017 |
71 |
Right Lateral Neck |
Superficial Spreading |
1 |
|
No |
|
64 |
Left Mid Helix |
Lentigo Maligna |
1 |
|
No |
|
91 |
Right Posterior |
Superficial Spreading |
4 |
2.0 |
Yes |
|
47 |
Left Abdo |
Superficial Spreading |
1 |
|
No |
|
84 |
Left Dorsal Ring |
Superficial Spreading |
1 |
|
No |
|
48 |
Right Anterior Neck |
Naevoid |
3 |
1.0 |
No |
|
69 |
Right Upper Back |
Lentigo Maligna |
1 |
|
No |
|
74 |
Left Superior |
Lentigo Maligna |
1 |
|
No |
|
61 |
Left Flank |
Superficial Spreading |
3 |
0.5 |
No |
|
70 |
Left Superior |
Superficial Spreading |
1 |
|
No |
|
65 |
Right Chest |
Superficial Spreading |
1 |
|
No |
|
75 |
Right Cheek |
Lentigo Maligna |
1 |
|
No |
|
51 |
Right Popliteal |
Lentigo Maligna |
1 |
|
No |
|
70 |
Right Chest |
Superficial Spreading |
3 |
0.5 |
No |
|
89 |
Left Lateral |
Lentigo Maligna |
1 |
|
No |
|
27 |
Right Mid Back |
Superficial Spreading |
2 |
0.6 |
No |
|
77 |
Right Upper Arm |
Superficial Spreading |
1 |
|
No |
|
77 |
Right Cheek |
Superficial Spreading |
1 |
|
Yes |
|
61 |
Left Mid Back |
Superficial Spreading |
1 |
|
No |
|
94 |
Right Cheek Medial |
Superficial Spreading |
1 |
|
No |
|
61 |
Right Upper |
Superficial Spreading |
1 |
|
Yes |
|
87 |
Right Lateral |
Lentigo Maligna |
1 |
|
Yes |
|
57 |
Right Postauricular |
Lentigo Maligna |
1 |
|
No |
|
52 |
Right Lateral Upper |
Lentigo Maligna |
1 |
|
No |
|
68 |
Left Upper Back |
Lentigo Maligna |
1 |
|
No |
|
73 |
Right Deltoid |
Lentigo Maligna |
2 |
0.3 |
No |
|
61 |
Right Deltoid |
Lentigo Maligna |
1 |
|
No |
|
56 |
Left Lateral Neck |
Superficial Spreading |
3 |
0.7 |
No |
2018 |
81 |
Left Abdo |
Superficial Spreading |
1 |
|
Yes |
|
86 |
Right Cheek |
Superficial Spreading |
1 |
|
Yes |
|
74 |
Left Parietal Scalp |
Nodular |
4 |
2.0 |
No |
|
69 |
Right Lateral |
Superficial Spreading |
1 |
|
Yes |
|
41 |
Left Abdo Medial |
Superficial Spreading |
2 |
0.3 |
No |
|
86 |
Left Posterior Calf |
Lentigo Maligna |
2 |
0.2 |
No |
|
62 |
Right Medial Calf |
Superficial Spreading |
2 |
0.2 |
No |
|
82 |
Right Frontal Scalp |
Lentigo Maligna |
3 |
1.0 |
No |
|
64 |
Left Superior |
Lentigo Maligna |
1 |
|
No |
|
72 |
Left Upper Back |
Lentigo Maligna |
1 |
|
No |
|
71 |
Right Cheek |
Lentigo Maligna |
1 |
|
No |
|
87 |
Right Deltoid |
Lentigo Maligna |
1 |
|
No |
|
96 |
Right Mid Helix |
Lentigo Maligna |
1 |
|
Yes |
|
76 |
Left Lateral |
Superficial Spreading |
1 |
|
No |
|
76 |
Left Lateral |
Superficial Spreading |
1 |
|
No |
|
82 |
Right Superior |
Superficial Spreading |
1 |
|
Yes |
|
48 |
Left Anterior |
Superficial Spreading |
1 |
|
No |
|
63 |
Left Lateral |
Superficial Spreading |
1 |
|
Yes |
|
68 |
Right Temple |
Lentigo Maligna |
1 |
|
Yes |
|
54 |
Left Upper Back |
Superficial Spreading |
1 |
|
No |
|
71 |
Left Cheek |
Lentigo Maligna |
1 |
|
No |
|
55 |
Right Lateral Neck |
Lentigo Maligna |
1 |
|
Yes |
|
46 |
Left Mid Back |
Superficial Spreading |
1 |
|
No |
|
90 |
Mid Glabella |
Lentigo Maligna |
1 |
|
Yes |
|
68 |
Right Cheek |
Lentigo Maligna |
1 |
|
Yes |
|
73 |
Right Chest |
Lentigo Maligna |
1 |
|
Yes |
|
97 |
Left Anterior Upper |
Lentigo Maligna |
1 |
|
Yes |
|
84 |
Left Cheek |
Lentigo Maligna and |
1 |
|
Yes |
|
72 |
Right Flank |
Lentigo Maligna |
1 |
|
Yes |
|
44 |
Left Deltoid |
Superficial Spreading |
1 |
|
Yes |
|
66 |
Right Superior |
Superficial Spreading |
2 |
0.2 |
No |
|
94 |
Left Lateral |
Superficial Spreading |
1 |
|
Yes |
|
66 |
Left Posterior |
Lentigo Maligna |
1 |
|
No |
|
48 |
Right Popliteal |
Superficial Spreading |
1 |
|
No |
|
56 |
Left Mid Back |
Superficial Spreading |
2 |
0.4 |
No |
|
61 |
Left Buttock |
Superficial Spreading |
2 |
0.3 |
No |
|
59 |
Mid Upper Back |
Lentigo Maligna |
1 |
|
No |
|
81 |
Left Angle Of |
Lentigo Maligna |
1 |
|
Yes |
|
54 |
Left Lateral Neck |
Lentigo Maligna |
1 |
|
No |
2019 |
63 |
Mid Parietal Scalp |
Lentigo Maligna |
1 |
|
No |
|
81 |
Left Angle Of |
Lentigo Maligna |
1 |
|
Yes |
|
79 |
Left Anterior Thigh |
Nodular |
5 |
6.8 |
No |
|
78 |
Right Upper Back |
Superficial Spreading |
1 |
|
No |
|
78 |
Left Mid Back |
Lentigo Maligna |
2 |
0.3 |
No |
|
78 |
Left Mid Back |
Superficial Spreading |
4 |
1.1 |
No |
|
28 |
Left Upper Back |
Superficial Spreading |
2 |
0.3 |
No |
|
49 |
Right Forehead |
Lentigo Maligna |
1 |
|
Yes |
|
66 |
Right Posterior |
Superficial Spreading |
4 |
2.0 |
Yes |
|
83 |
Right Tip Of The |
Lentigo Maligna |
1 |
|
No |
|
41 |
Right Anterior Shin |
Superficial Spreading |
1 |
|
No |
|
87 |
Mid Tip Of The |
Lentigo Maligna |
1 |
|
No |
|
72 |
Right Deltoid |
Lentigo Maligna and |
1 |
|
Yes |
|
55 |
Right Tip Of The |
Lentigo Maligna |
1 |
|
Yes |
|
66 |
Right Anterior |
Lentigo Maligna |
1 |
|
No |
|
61 |
Left Upper Back |
Superficial Spreading |
1 |
|
Yes |
|
65 |
Left Lateral |
Superficial Spreading |
1 |
|
No |
|
57 |
Left Upper |
Lentigo Maligna |
1 |
|
Yes |
|
57 |
Right Posterior |
Lentigo Maligna and |
1 |
|
Yes |
|
76 |
Right Temple |
Lentigo Maligna |
1 |
|
Yes |
|
55 |
Left Anterior Shin |
Superficial Spreading |
1 |
|
Yes |
|
74 |
Left Cheek |
Lentigo Maligna and |
1 |
|
Yes |
|
67 |
Mid Lower Dorsal |
Lentigo Maligna |
1 |
|
Yes |
|
41 |
Left Mid Back |
Lentigo Maligna and |
1 |
|
Yes |
|
56 |
Right Upper Back |
Nodular |
4 |
2.5 |
No |
2020 |
85 |
Right Deltoid |
Lentigo Maligna |
1 |
|
Yes |
|
81 |
Right Lateral Neck |
Superfical Spreading |
2 |
0.3 |
No |
|
53 |
Right Mid Back |
Nodular |
4 |
1.5 |
No |
|
52 |
Right Mid Back |
Lentigo Maligna |
1 |
|
No |
|
38 |
Left Mid Back |
Superfical Spreading |
1 |
|
No |
|
45 |
Right Chest |
Superfical Spreading |
2 |
0.3 |
No |
|
44 |
Right Preauricular |
Lentigo Maligna |
1 |
|
No |
|
74 |
Right Mid Back |
Superfical Spreading |
3 |
0.6 |
Yes |
|
76 |
Right Flank |
Superfical Spreading |
2 |
0.3 |
No |
|
78 |
Left Flank |
Superfical Spreading |
4 |
3.0 |
No |
|
64 |
Right Upper Back |
Superfical Spreading |
2 |
0.4 |
No |
|
68 |
Right Lower Cheek |
Lentigo Maligna |
1 |
|
Yes |
|
70 |
Left Cheek |
Lentigo Maligna |
1 |
|
No |
|
69 |
Right Lower Back |
Lentigo Maligna |
1 |
|
No |
|
73 |
Left Posterior Neck |
Desmoplastic |
4 |
2.0 |
No |
|
80 |
Left Vertex |
Superfical Spreading |
2 |
0.4 |
No |
|
67 |
Left Cheek |
Lentigo Maligna |
2 |
0.2 |
Yes |
|
85 |
Left Posterior Shoulder |
Superfical Spreading |
1 |
|
Yes |
|
47 |
Left Inner Upper |
Superfical Spreading |
3 |
0.7 |
No |
Total |
141 |
|
|
|
|
|
Age |
Number of Cases |
Percentage |
10 |
0 |
0% |
20 |
4 |
2.8% |
30 |
2 |
1.4% |
40 |
18 |
12.8% |
50 |
21 |
14.9% |
60 |
36 |
25.5% |
70 |
31 |
22.0% |
80 |
21 |
14.9% |
90 |
8 |
5.7% |
Clark level |
|
|
Level 1 |
98 |
69.5% |
Level 2 |
23 |
16.3% |
Level 3 |
10 |
7.1% |
Level 4 |
9 |
6.4% |
Level 5 |
1 |
0.7% |
Melanoma Subtype |
|
|
Superficial spreading |
72 |
51.1% |
Lentigo maligna |
56 |
39.7% |
Superficial spreading and lentigo maligna |
5 |
3.5% |
Nodular |
4 |
2.8% |
Amelanotic nodular |
2 |
1.4% |
Naevoid |
1 |
0.7% |
Desmoplastic |
1 |
0.7% |
Location of melanoma |
|
|
Face |
35 |
24.8% |
Back |
26 |
18.4% |
Arm |
18 |
12.8% |
Leg |
18 |
12.8% |
Neck |
11 |
7.8% |
Shoulder |
9 |
6.4% |
Abdomen |
8 |
5.7% |
Chest |
5 |
3.5% |
Scalp |
4 |
2.8% |
Ear |
4 |
2.8% |
Buttock |
2 |
1.4% |
Hand |
1 |
0.7% |




































