Open Access
Research Article
Max Screen
ISSN: 2770-839X
Copyright: © 2021 Zakaryaa S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Introduction: Cutaneous adnexal carcinomas are rare cutaneous malignant adnexal tumors derived from eccrine and apocrine sweat glands, follicular structures and sebaceous glands. They represent less than 1% of cutaneous cancers
Porocarcinoma and hidradenocarcinoma are two main types of eccrine sweat carcinomas of unknown pathogenesis characterized by their clinicopathological diversity.
Porocarcinoma is a rare malignant tumor (< 0.01% of skin tumors) derived from the intraepidermal portion of the eccrine sweat duct: the acrosyringium, occurring de novo or after degeneration of an eccrine poroma.
Hidradenocarcinoma is a rare malignant sweat tumor representing 0.001% of all tumors, classically arising de novo and more rarely after degeneration of a pre-existing benign hidradenoma.
Results: We report 4 cases of sweat adnexal carcinomas of various locations and clinical aspects including 2 cases of hidradenocarcinoma and 2 cases of eccrine porocarcinoma that were initially diagnosed as melanoma or squamous cell carcinoma.
The diagnosis required, in addition to the histological study, a complementary immunohistochemical study.
The optimal treatment, in the absence of distant extension, consisted of wide tumor resection with safety margins, completed by adjuvant radiotherapy in a patient with lymph node extension and by palliative chemotherapy in a patient diagnosed at the stage of pulmonary metastases.
All the clinical, paraclinical and histological characteristics as well as the therapeutic management of each patient were reported in this study.
Discussion: Porocarcinoma and hidradenocarcinoma are rare adnexal tumors of the sweat glands with a local aggressive power and a non-negligible metastatic potential as well as a frequent risk of local recurrence.
The diagnosis is based on histological and immunohistochemical studies.
The early management, whose mainstay is wide tumor resection with safety margins, determines the prognosis.
The great variety of adnexal carcinomas, their rarity, their non-specific clinical presentation as well as the difficulty of histological diagnosis represent the interest and originality of our study.
Keywords: Adnexal Carcinomas; Porocarcinoma; Hidradenocarcinoma
Cutaneous adnexal carcinomas are rare cutaneous malignant adnexal tumors derived from eccrine and apocrine sweat glands, follicular structures and sebaceous glands [1]. They represent less than 1% of cutaneous cancers [2].
Porocarcinoma and hidradenocarcinoma are two main types of eccrine sweat carcinoma with unknown pathogenesis and characterized by their great clinicopathological diversity [3].
Porocarcinoma is a rare malignant tumor (< 0.01% of skin tumors) first described by Pinkus and Mehregan in 1963 as an epidermotropic eccrine tumor [4].
The term « porocarcinoma » was introduced in 1969 by Mishima and Morioka who identified that it derives from the intraepidermal portion of the eccrine sweat duct: the acrosyringium; occurring de novo or after degeneration of an eccrine poroma [5]. Since then, less than 500 cases of porocarcinoma have been described in the literature [6].
On the other hand, hidradenocarcinoma is also a rare malignant sweat tumor representing 0.001% of all tumors, occurring classically de novo and more rarely after degeneration of a pre-existing benign hidradenoma [7].
These tumors can sometimes present a diagnostic and therapeutic problem and have a significant potential for locoregional and metastatic dissemination if diagnosed and managed late [8-10].
We report 4 cases of adnexal sweat carcinomas of various locations and clinical aspects including 2 cases of hidradenocarcinoma and 2 cases of eccrine porocarcinoma that were initially diagnosed as melanoma and squamous cell carcinoma.
All the clinical, paraclinical and histological characteristics as well as the therapeutic management of each patient were reported in this study.
A 64-year-old patient with a history of chronic smoking presented a painless nodule of the right heel that had appeared 2 years ago and had progressively increased in size complicated by ulceration.
Clinical examination revealed a rounded tumor mass measuring 5 cm in long axis with ulcerated center associated with a magma of right inguinal adenopathies (Figure 1).
The patient underwent a large tumor resection. The histological study showed a malignant tumor proliferation infiltrating the dermis and ulcerating the epidermis arranged in lobules, made of clusters of clear cells within a hyaline, fibrous and inflammatory stroma. Atypia and mitoses were frequent associated with lymphatic emboli.
The immunohistochemical study showed that the cells strongly expressed cytokeratin 17 and epithelial membrane antigen (EMA). It also showed a focal positivity of cytokeratin 7 (CK7) in the superficial ductal structures with a strong expression of PHLDA1, a follicular and sweat marker. Thus, the histological and immunohistochemical appearance was in favor of a hidradenocarcinoma.
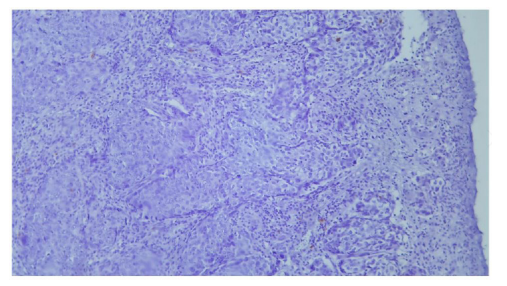
The patient also underwent homolateral lymph node dissection. The histological study revealed tumor- infiltrated nodes with capsular invasion (Figures 2 and 3).
The patient underwent a complementary radiotherapy with a good evolution without any recurrence during 34 months.
A 68-year-old patient, farmer, had a history of arterial hypertension, chronic smoking, and a squamous cell carcinoma of the left arm for which he benefited from a tumor removal 2 years ago.
He presented a recurrence of a painful ulcerated lesion at the site of the biopsy removal that was progressively enlarging until it formed a circumferential lesion on the left arm evolving in a context of altered general condition (Figure 4 and 5).
On clinical examination, it was an erosive circumferential placard taking the upper 2/3 of the left arm, with multiple nodules and irregular pigmented borders.
The rest of the examination revealed a right homolateral axillary adenopathy measuring 4 cm, firm and painless, with no inflammatory signs, associated with a painful limitation of the articular amplitudes of the left shoulder.
The rest of the clinical examination didn’t reveal any abnormalities.
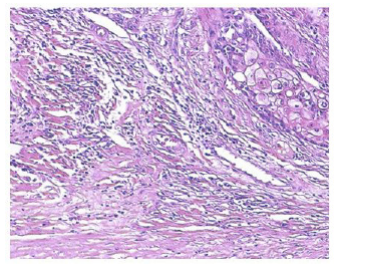
The patient underwent a skin biopsy which revealed poroid differentiation in favour of a porocarcinoma with positive labelling for CEA and not for EMA (this is not an absolute criterion). This malignant adnexal tumor showed basaloid and epidermoid differentiation (Figures 6 and 7).
The diagnosis retained was eccrine porocarcinoma.
The extension workup revealed necrotic left axillary adenopathies and a small amount of pleurisy.
The therapeutic management was palliative with a polychemotherapy: 5 FU (fluorouracyl) - CDDP (cisplatin).
An 80-year-old patient with a history of arterial hypertension and chronic smoking presented a nodular lesion on the inner side of the left thigh that had appeared 4 years earlier, progressively increasing in volume and becoming bleeding on contact 2 months before admission.
Dermatological examination revealed an erythematous nodular lesion measuring 2 cm in long axis, with irregular margins, smooth surface and bleeding on contact (Figures 8 and 9).
An initial skin biopsy was in favor of a melanoma but immunohistochemistry was not performed. The extension workup didn’t reveal any abnormalities.
Treatment consisted of tumor removal with 2 cm resection margins.
The histological study revealed a tumor proliferation reaching the epidermis and invading the dermis with large tumor cells, a high nucleo-cytoplasmic ratio, multiple mitotic atypia (Figure 10).
Immunohistochemical study showed that the tumor cells were positive for CkAE1/CkAE3, EMA; they were negative for CEA and for melan. A, HNB45, PS100 (Figures 11 and 12).
The retained diagnosis was porocarcinoma
A 61-year-old patient with a 15-year history of vitiligo presented an inguinal nodule that had appeared since the age of 14 and had been increasing rapidly in size during 2 years, complicated by ulceration and bleeding on contact.
Dermatological examination revealed a firm erythematoviolet nodular lesion with irregular borders measuring 6 cm in long axis, ulcerated in places and surmounted by a small nodule of 1 cm.
A skin biopsy with histological and immunohistochemical study revealed an atypical hidradenoma with high proliferation index focally in depth without sufficient arguments of malignancy, with CEA and EMA labeling (Figure 13).
There was no extension to other locations.
The patient underwent a tumor resection with anatomopathological study revealing a malignant tumor proliferation with sweat differentiation, high ki67, multiple nuclear atypia.
The retained diagnosis was a hidradenocarcinoma on pre-existing hidradenoma.
Hidradenocarcinoma is a rare malignant sweat tumor representing less than 0.001% of all tumors. To date, less than 100 cases have been described in the literature [10]. They occur in the sixth and seventh decades with a slight preponderance among females [11].
Porocarcinoma is also a rare sudoral carcinoma representing between 0.005% and 0.01% of malignant skin tumors [12].
Both of these eccrine adnexal sweat tumors usually occur after the 6th decade with no gender predominance and the main risk factors are chronic sun exposure, exposure to chemical agents and immunosuppression. Genetic abnormalities are beginning to be described, notably a t (11 ; 19) translocation and mutations of p53 [2].
They can appear de novo or following degeneration of benign adnexal tumors (hidradenoma or eccrine poroma) [2].
The sites of predilection are represented by the head and neck as well as the extremities where the tumor can have various clinical manifestations: nodular, budding or even in the form of a plaque that can ulcerate secondarily ; this can lead to confusion with other types of cutaneous cancers, in particular basal cell carcinoma, cutaneous squamous cell carcinoma, achromic melanoma ... [13].
In addition to the varied clinical manifestations of sweat carcinomas, the histological diagnosis is also difficult and requires an immunohistochemical study to look for the expression of glandular markers (ACE, EMA...) [14].
Their treatment is based on wide tumor removal + /- supplemented by radiotherapy at the site of lymph node drainage or by polychemotherapy at the metastatic stage (doxorubicin, cyclophosphamide, cisplatin, vincristine, bleomycin...) [15].
These adnexal sweat carcinomas have a poor prognosis if managed late, with a non-negligible risk of metastasis and recurrence that can reach up to 20% of cases, as well as a high mortality rate in case of metastatic involvement.
Although rare, hidradenocarcinoma and porocarcinoma can sometimes present a diagnostic and therapeutic problem. The diagnosis is based on histological and immunohistochemical studies. The early management, whose mainstay is wide tumor resection with safety margins, determines the prognosis, the risk of local recurrence and prevents the occurrence of locoregional and distant extension. Thus appears the interest to evoke them in front of any suspected cutaneous carcinoma.

![]()

 |
| Figure 1: Clinical image of erythematous, hyperkeratotic papule on the left distal dorsal middle finger |
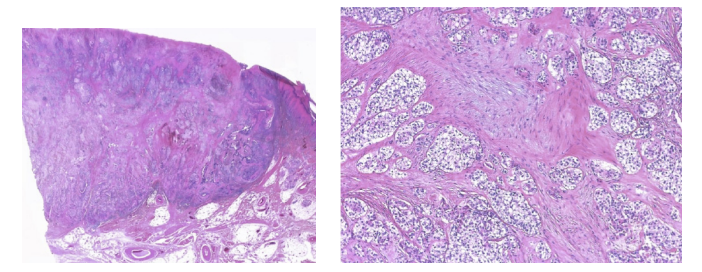 |
| Figure 2 and 3: Histological appearance of hidradenocarcinoma |
 |
| Figure 4 and 5: Erosive circumferential plaque covering 2/3 of the left arm with multiple nodules with irregular pigmented borders |
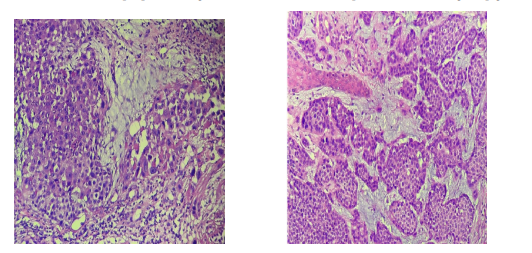 |
| Figure 6 and 7: Histological appearance of a carcinomatous proliferation suggesting a porocarcinoma |
 |
| Figure 8 and 9: Erythematous nodular lesion measuring 2 cm in long axis, with smooth surface, with irregular hyperpigmented edges |
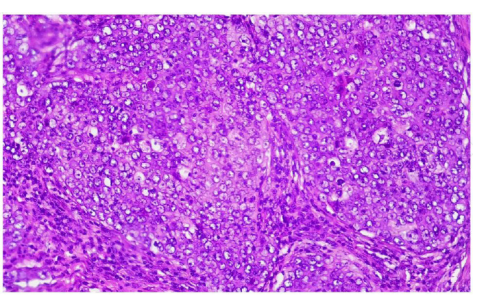 |
| Figure 10: Histological aspect of the tumoral lesion |
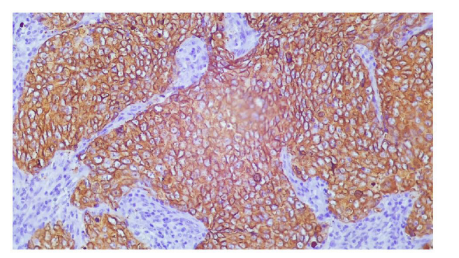 |
| Figure 11: Immunohistochemistry: Cytokeratin A2/A3 positive |
 |
| Figure 12: Immunohistochemistry: HMB45 negative |
 |
| Figure 13: Histological aspect of hidradenocarcinoma |




































