Open Access
Research Article
Max Screen
ISSN: 2770-839X
Copyright: © 2021 Zhu CS. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Dermatofibroma (DF) is a common benign fibrosing lesion that can be found on any surface of the body, most often in the lower extremities. Dermatofibroma that arises on the digits, as in our present case, may be confused with other clinical entities or even malignant tumors, leading to unnecessarily aggressive treatment.To ensure proper diagnosis and treatment, dermatofibroma should be considered in the differential diagnosis of digital papules.
Keywords: Digital Dermatofibroma; Cutaneous Fibrous Histiocytoma; Skin Growth
List of abbreviations:DF: Dermatofibroma; CD: Cluster of Differentiation; SMA: Smooth Muscle Actin; EMA: Epithelial Membrane Antigen; NSE: Neuron Specific Enolase
Dermatofibroma (DF), also known as cutaneous fibrous histiocytoma, is a common benign fibrosing lesion that can be found on any surface of the body, most often in the lower extremities [1-3]. Here, we describe a rare presentation of digital dermatofibroma.
An otherwise healthy man in his 30s presented with a chief complaint of a papule on his left middle finger (Figure 1). The lesion was moderately painful and had been enlarging over a year and a half. The lesion had not been treated in the past and there was no history of antecedent trauma. The patient’s medical history was unremarkable, and he had no history of skin cancer. Physical examination revealed an erythematous, hyperkeratotic papule on the dorsal surface of the left middle finger (Figure 1). Shave biopsy was performed and sent for histology (Figures 2 and 3).
Histopathologic sections revealed fascicles of plump fibroblasts and histocytes interposed between thick collagen bundles in the dermis. A rare normal-appearing mitotic figure was identified. Immunohistochemical staining was negative for CD34, AE1/AE3, SMA (smooth muscle actin), and EMA (epithelial membrane antigen), but positive with CD10 and Factor XIIIa stains. Ki-67 staining showed relatively low (10-15%) proliferation index. A diagnosis of dermatofibroma was made and given the broad extension of the lesion to the base of the specimen, the lesion was removed by electrodesiccation and curettage without recurrence.
Dermatofibroma presents as single or multiple papules or nodules that characteristically demonstrate the “dimple sign” when squeezed and can have a smooth, plaque-like, or umbilicated surface. DF can range from 2 to 14 mm in diameter, with an average size of 7.3 mm and is often described as a firm, mobile papule that is non-adherent to underlying subcutaneous tissue. DF is commonly found in early to mid-adulthood and may arise following some form of trauma, such as a ruptured hair follicle or insect bite [1-4]. It is theorized that an inflammatory response develops to the initial insult, followed by a fibrous reparative process [4]. Along with the aforementioned clinical findings, the diagnosis of DF can also be assisted by use of dermoscopy, which can show a variety of presentations but most commonly demonstrates a central white patch with a peripheral pigment network [2].
While dermatofibromas can often be clinically diagnosed, histopathology remains the gold standard for diagnosis, especially in rare presentations of digital dermatofibroma, which may be confused with a variety of benign and malignant entities, including cellular digital fibroma, acral fibrokeratoma, leiomyosarcoma, and dermatofibrosarcoma protuberans [1,2,4]. Also in the differential is orf, a skin infection caused by a Parapox DNA virus that commonly manifests on the hands and can resemble digital dermatofibroma [5].
On histopathology, dermatofibroma is composed of fibrocytes primarily located in the dermis with occasional extension into the subcutis. Macrophages can be found, along with a mixture of other inflammatory cells, including giant cells, lymphocytes, neutrophils, plasma cells, eosinophils, and mast cells. Coarse collagen bundles are also typical of dermatofibroma, as is an induced hyperplasia of nearby structures such as the epidermis, hair follicles, and melanocytes [1-3].
Immunohistochemical staining of dermatofibroma is variable depending on the age of the lesion. Macrophage markers and factor XIIIa markers are strongly positive in early lesions although reactivity of the latter tends to diminish as the lesion ages. Lysozyme, trypsin, and chymotrypsin markers react inconsistently. Early dermatofibroma may be rapidly evolving, demonstrating an elevated proliferation index with markers such as Ki-67. Other reported but variably expressed markers include smooth muscle-specific actin, NKIC3, NSE (neuron-specific esterase), factor VIII, and rarely, S100 protein [3].
Treatment is often not necessary for dermatofibroma but can be considered for symptomatic lesions or for cosmetic purposes. Several therapies exist, with varying results, including cryotherapy, superficial shaving, intralesional steroid injection, and pulsed dye laser. Surgical excision can effectively treat this benign lesion, but results in scarring [6].
The dermatofibroma in our case presented in an unusual location on the digit, where it may easily be confused with other clinical entities such a verruca vulgaris, pyogenic granuloma, or even malignant tumors, leading to unnecessarily aggressive treatment [1]. To ensure proper diagnosis and treatment, dermatofibroma should be considered in the differential diagnosis of digital papules.
None

![]()

 |
| Figure 1: Clinical image of erythematous, hyperkeratotic papule on the left distal dorsal middle finger |
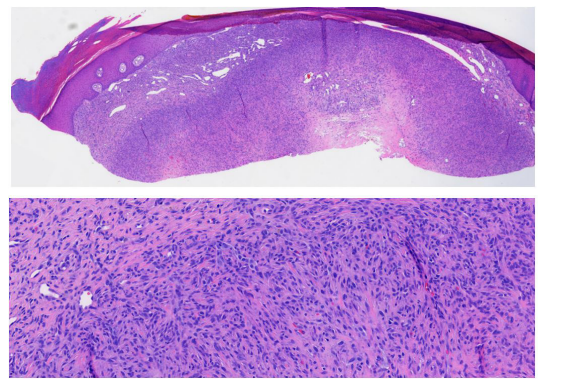 |
| Figure 2 and 3: H&E 4x and 20x. Histopathologic sections revealed fascicles of plump fibroblasts and histocytes interposed between thick collagen bundles in the dermis |




































