Open Access
Research Article
Max Screen
ISSN: 2770-839X
Copyright: © 2019 Hewageegana HGSP. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objective:Ayurveda has discussed all skin diseases under the name of Kushtha, and in other words it can be known as “Ayurveda Dermatology”. Eighteen types of these skin diseases are mainly divided into seven types of Maha Kushtha and eleven types of Kshudra Kushtha. Vipadika skin disease is diagnosed with the help of critical and analytical study of the literature in original Sanskrit texts and later clinical trial was carried out. In the present study, efficacy of Vipadikahara grita taila was assessed against Vipadika skin disease.
Method:Vipadikahara grita taila was used as the test drug and tested first time in a clinical study without internal treatment regimen. Clinical research was conducted using 100 patients (n=50/treated group and n=50/control group). Patients were identified based on clinical symptoms of Vipadika skin disease and registered them from outdoor and indoor patients’ departments of Ayurveda Teaching Hospital, Borella, Sri Lanka.
Result:A significant reduction of the symptoms such as itching, splitting and pain were identified as a result of its high medicinal value
Conclusion:Vipadika kushtha treated with Vipadikahara grita taila displayed a significant improvement of wound healing and the oil is an effective, easily and applicable, successful, user friendly, pleasant odor medicated oil.
Keywords: Skin Disease; Kushtha; Vipadika; Clinical Study; Vipadikahara Grita Taila
Skin diseases are common in the world and any discoloration or weakness at the skin becomes a great handicap for a person in the society [1]. According to Ayurveda, eighteen types of skin diseases come under “Kushtha” [2]. Ayurveda treatments are very popular for skin diseases among Sri Lankans. When considering the etiopathogenisis, it was apparent that all main texts had mentioned almost same process. According to Caraka Samhita [3], first etiological factors vitiate three humors; Vata, Pitta and Kapha as well as four tissues; blood, skin, muscle tissue, plasma simultaneously. In Susruta Samhita [4], it was different to some extent such as: by the causative factors, Pitta and Kapha become aggravated first and then Vata associate with these two humors and become increased. Then those humors go deep inside by vitiating the tissues. According to Ashtangahrida Samhita [5], initially increase or aggravate the humors by etiological factors. Then the vitiated three humors move inside through the horizontal blood vessels to the relaxed tissues blood, skin, muscle tissue, plasma and making them loose (weak). However, it is clear that the disease Kushtha is originated with vitiation of one, two or all three humors.
There are many preliminary symptoms for Kushtha was pointed out in the Ayurveda texts but symptoms such as loss of sweating, excessive sweating, roughness of the skin, colour changes of the skin, itching, pain, skin fissures, burning sensation, horripilation are common for all types of skin diseases including Vipadika. In view of Vipadika skin disease, it was come under Kshudra kushtha and as one of the Vataja nanatmaja vikara (disease mainly caused by Vata dosha) according to Caraka samhita Sutra chapter [3]. Acarya Caraka was mentioned the symptoms of Vipadika skin disease in Cikitsa chapter as bursts in feet and hands, fissures in feet and hands with acute pain are as main symptoms. Acarya Dalhana; a commentator to Susruta samhita cited that dark streaks, rough to feel, itching, painfullness, increased tone as symptoms and these may be present at either in palms or in feet [6].
A large number of people in the community suffer from skin diseases. When considering about the prevalence of skin diseases in Sri Lanka, studies conducted by the year of 2000 with some of the provincial and general hospitals records shows all these dermatitis/eczemas constituted the largest group (42.6%-32.3%) [1]. However, there is no clear records relate to Vipadika skin disease though it is very common type of skin disease present clinically in Sri Lanka with above mentioned symptoms. Numbers of medicated oils are mentioned in Ayurveda original texts for various types of skin diseases. Some of them contain large number of ingredients and have to follow complex preparation methods. Abhyanga with various Sneha Dravya are commonly practiced in the treatment of Vipadika Vipadikahara grita taila (VHGT) is specific medicated oil for external application: mentioned in Caraka Samhita in Kushta chikitsa to treat five types of skin diseases such as, Vipadika, Carma kushta, Eka kushta, Kitibha and Alaska [3]. However, it is specific among them for Vipadika Kushtha as the ingredients of the oil help to heal the cutting or bursting wounds. There are no previous studies on management of Vipadika skin disease only using external application. In the present study, an attempt was taken to clinically evaluate the efficacy of Vipadihkahara ghrita taila against Vipadika skin disease.
Vipadikahara ghrita taila contains four medicinal plants [Leptadenia reticulata (Retz) Wight and Arn., (Family: Asclapadaceae), Rubia cordifolia Linn Syst., (Family: Rubiaceae), Berberis aristata DC. Syst., (Family: Berberidaceae), Mallotus Philippensis (Lam.) Muell. Arg. (Family: Euphorbiaceae)], two liquids (cow’s milk and the water), two oils (cow’s ghee and Sesame oil), resin of Soria robusta Geartn.f. (S. robusta) and bee’s wax [3]. In brief, a decoction was prepared by using equal amounts (120 g/ each) of three medicinal plants: Leptadenia reticulate (whole plant), Rubia cordifolia (stem) and Berberis aristata (stem) adding 1440 ml of water. It was heated using mild flame until the volume of water was reduced to one fourth (360 ml) of the original volume. Then cow’s milk 1440 ml was added to the decoction and allowed to reduce the volume further. After that, mixture was filtered through a muslin cloth. Then Sesame oil and cow’s ghee (720 ml each) were added in to filtrate. When gradually reduced the volume, the paste (glands and hairs of the fruit of Mallotus Philippensis) 90 g was added to the oil and stirred well. Later, boiled it in mild flame until reduces the volume while stirring well continuously to avoid the adhesion to vessel. When the oil became froth less, filtered using a clean cloth. Lastly, bee’s wax and resin of S. robusta (5g each) were added when the oil was hot.
This medicated oil was red due to R. cordifolia and red glands and hairs of M. phillipinensis. The characteristic odor is due to the ghee and sesame oil, which were used as the oil base. Furthermore, Vipadikahara ghrita taila was standardized using quality assessment protocols [7]. Placebo was the oil base of Vipadikahara ghrita taila (properly mixed, equal amounts of ghee and Sesame oil). Preparations were kept in clean airtight containers until used.
Ethical approval for the clinical trial was granted under the registration Number of ERC 12/06 by the Ethical Review Committee of Indigenous Medicine, University of Colombo, Rajagiriya, Sri Lanka.
Clinical research was conducted using 100 patients (n=50/treated group and n=50/control group). Patients were identified based on clinical symptoms of Vipadika skin disease and registered them from outdoor and indoor patients’ departments of Ayurveda Teaching Hospital, Borella, Sri Lanka. Some patients who are in very remote areas and difficult to attend the clinics regularly were admitted to the hospital and completed the treatment.
Patients, age between 20-70 years with the symptoms of Vipadika skin disease in both males and females were selected to continue the research. Participants were having inadequate response to Allopathic medicine, symptoms for at least 03 months and willing and able to comply with all study procedures for the duration of the study were selected.
Patients who have symptoms merged with other types of Kushtha, suffering with diabetes mellitus, hypertension, chronic lung diseases, malignancies, long term treatment with topical steroids for the skin disease, subjects who are not competent in giving consent, pregnant and lactating mothers (oil applies on palms or plantar surface or in both during the trial and though it is an external application there may be a risk to pregnancy or breastfeeding mothers because it can be absorbed to the body via skin), subjects who had sensitivity reactions to the medicated oils, and Vipadika skin disease with secondary infections were excluded.
The study was conducted using a prospective, randomized design. The suitable subjects were selected in accordance with computer generate random number list (n=50/group). Sample size was calculated according to the method given in WHO practical manual [8].
N = Sample size
Z = Critical value of 95% confidence interval (1.96)
D = Absolute percentage (5%)
P = Expected prevalence of skin disease cases present in Ayurveda Clinic in Borella Ayurveda Teaching Hospital (3%)
Patients who are consenting to study and satisfying the study criteria will be recruited according to the following sample size calculation.
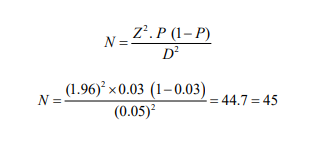
Expected dropouts = 10%
Minimum sample size = 45 + 5 = 50 for one arm
Participants were treated with Vipadikahara grita taila or placebo for 6 weeks. The study medications were applied twice a day (morning and evening). Group A (Treated group): participants were treated with Vipadikahara grita taila and they advised to apply the oil only on the lesions only after washing by luke warm water and drying. Group B (Control Group): placebo (ghee and Sesame oil) was used for control group and same procedure was followed as group A.
Vipadikahara grita taila or placebo was given to the patients in tightly sealed containers to minimize the contamination. Patients were advised not to apply any other remedy on the skin lesion during study period and also not to apply the test drug or the control on the day of assessment. Volume of the Vipadikahara grita taila or placebo given to the patients is depend (minimum 45 mL) according to the area of the skin lesion.
Patients in the inclusion criteria were informed about the study design. They could stop the treatment at any time without any discrimination. Written consent from each patient was obtained. The nature, aim, procedures, benefits and the possible risks of the study were explained to the eligible participants. Verbal consents were obtained prior to the screening. Medical history and the clinical examination were considered as baseline records for screening test. Patients also subjected to routine and special laboratory examinations: Random blood sugar (RBS), Blood urea, Urine Full Report (UFR), White Blood cell Count (WBC) and Erythrocytes, Sedimentation rate (ESR). These tests were carried out before and after the treatment to rule out other associate pathology and as well as to assess the effect of the therapy. The clinical examination was done following a specially prepared proforma.
A demonstration was conducted to the patients regarding application of the Vipadikahara grita taila or placebo over the affected area. Patients were reviewed once a week at the clinic in Ayurveda Teaching Hospital. Subjects were instructed to maintain the patient’s information form daily by recording progress and any adverse effect since using the Vipadikahara grita taila or placebo and also advised, if any adverse effect is noticed, it should be reported back to the investigator soon. The patients also had to be willing and able to complete self assessment scales as part of the assessment visits.
Assessment criteria were based on effect of the treatment or placebo in each group of 50 participants after completing their six weeks evaluation period. Thus, evaluation was based on the reduction of the cardinal symptoms. Physical findings were evaluated before treatment, during the treatment and after treatment
Measurement of length, depth and the width of the fissures were taken every other week during the period of application. One or more than 1 cm lengthy fissure wounds were measured and calculated. Slight cracks were ignored.
Linear measurement: simple dimensional assessment was performed in cutting or splitting wounds using a polythene piece keeping on the foot/palm of the patient and marked them. Later, lengths (in mm) of the fissures were measured and calculated (in cm) using plastic flexible ruler. Length is the longest distance of a wound margin to margin. The second measurement (width) is made perpendicular to the length (also at the widest distance). When measuring the width, placed the ruler over the widest aspect of the wound and measured from 3 o’clock to 9 o’clock according to Wendelken and co-workers [9].
When measuring depth, a cotton-tip applicator was placed into the deepest part of the wound bed. Then grasped the applicator by the wound margin and placed it against the ruler and reading was taken [10]. Same units were used to measure and calculate the width and the depth. In addition, healing of wounds was evaluated by measuring reduction of the length, width, depth and number of ulcers once a week.
Assessment criteria and scoring system was developed to evaluate the symptoms (subjective criteria) at the site of the skin lesion. Itching, roughness, cracking, pain, swelling, burning sensation in affected site, eruption of papules, exudates type, colour changes and general symptoms (fever, lymph enlargement) were examined and evaluated before, during and after the treatment as described by Hewageegana and co-workers [11]. In addition to that, Photographs were taken before and after the treatment. At the beginning of the trial, all selected participants were advised to complete the trial as this treatment was easy and safe method of management for Vipadika kushtha.
Overall results related observations of individuals were done as follows:
1. Complete remission: 100% relief or patient did not complain any signs or symptoms relate to Vipadika skin lesion such as itching, roughness, cracking of the skin again and again, pain, swelling, burning sensation in affected site, eruption of new papules, secretions from particular area, no remaining of colour changes and general symptoms.
2. Marked improvement: More than 76% above mentioned signs and symptoms were cured at the end of the treatment
3. Moderate Improved: Improved the above mentioned signs and symptoms between 51-75% at the end of the treatment.
4. Improved: Improved the above mentioned signs and symptoms between 26-50% at the end of the treatment.
5. Unchanged: Below 25% relief of the signs and symptoms
After completing the treatment, all patients were kept further three-month under the supervision as follow-up study.
At the beginning, patients were selected using computer generated numbers and odd numbers were used for the treated group and equal numbers for control group. Proforma was filled for each patient before starting the treatment. During the treatment, all patients were observed once a week and mentioned the changes of the skin lesion [with the help of patient’s form] and the other symptoms.
The score differences on day 1 and after 6 weeks for observed clinical signs were calculated for both groups separately and compared statistically using Mann Whitney u test. The results were expressed as mean ± SEM. Finding of P< 0.05 were considered to indicate statistical significance. Symptoms of Vipadika Kushtha were assessed according to the assessment score and there mean score was calculated. Then it was given in % reduction for further clarification.
In clinical study, 100 patients were compelled to complete the trial both in treated and control groups and analysis of demographic data showed that 34% of the patients were between 41 - 50 years (middle age), but it was not significant comparing with the other age distribution and it may due to start of the vitiation of Vata humor with the age. Sex wise distribution, religion and marital status do not show significant effect to occurrence Vipadika skin disease. According to the dietary habits, 21% of were vegetarian and 79% were non-vegetarian. Therefore, a significant difference was observed with dietary patterns. Caraka Samhita pointed out the connection between food habits and skin diseases under the etiological factors of Kushtha [3]. Hence, it is logical that people who are non-vegetarian have more prone to vitiation of Vipadika skin disease and other skin diseases with vitiation of all three humors. But the results did not show any difference between veg and non-veg groups directly when curing the fissures. There is no significant difference in the patients with high and low education levels, good and poor socio economic condition and hygienic conditions and unhygienic conditions. Therefore, they do not directly connect with Vipadika skin lesion. Vipadika skin disease is appeared not only in the feet but can be seen in both palms and feet or either in palms or in feet [3]. Therefore, strenuous work such as walking long distance, heavy work do not cause direct influence to vitiate relevant humors to initiate the Vipadika skin disease.
Normally, this disease is chronic (61% of the patients have been suffering more than 07 months) and this indicates the frequency of exacerbations and remissions with the treatment and difficulty for complete recovery. According to Kushtha treatment in Bhela Samhita [12], Vipadika skin disease comes under nine incurable Kushtha even though medical treatments were given. However, Vipadika skin disease is hard to cure due to it’s humors and chronicity.
When considering about the etiological factors, only 17% patients had contact history with chemicals or detergents and therefore, chemicals may not influence Vipadika skin disease directly. Forty seven per cent patients are having Vata kapha body constituents. According to Gangadhara commentary of Caraka Samhita, treatment chapter [3], Vipadika skin disease is mainly Vata kapha predominant disorder, but all three humors are connected to origin the Kushtha at the beginning or in different stages are unavoidable. Therefore, special characters related to other two humors: Pitta and Kapha were also seen in all patients. Therefore, persons with Vata kapha body constituents are more prone to get Vipadika skin disease than others.
When considering about mental conditions of the patients (Mano guna), 68.0% were with Rajas guna predominant. Rajas guna connects with Vata humor. Tamas guna is connecting with Kapha humor. When rajas or tamas mental condition is predominant, they can predispose to imbalance and ill health [13]. Accordingly, these patients may play a major role in manifestation of skin diseases also.
There is no direct connection to toxic morbid metabolic waste material (Ama) formed due to improper digestion and with passing of hard stools in Vipadika skin disease. Thirty five per cent of patients complained food allergy for beef/red meat/salmon, 32% for pickle/vinegar preparations and 27% for tomato, pineapple and mango and those food tend to increase the disease also. However, patients did not consume above foods after recognizing the possibility to increase the disease. According to texts, indulgence in incompatible food, i.e. person who uses cold and hot things simultaneously, is contradictory to Vatadi three humors [3], improperdiet and regime according to Susruta Samhita [6], incompatible food [5], Person who eats food mutually contraindicated [12,13] is helpful to develop skin diseases. These factors are very apparent when concidering with the results of the clinical study. Patients were unable to done their day today work due to pain of the fissures, papules, swelling in palms or feet and general symptoms of the body.
Hematological parameters such as WBC count, RBC count, and blood urea levels, fasting blood sugar levels and the specific gravity of urine were did not change significantly before and after the treatment in both treated, and control groups (Table 1).
Patients of treated group showed good response and significant improvement of the symptoms: itching, fissures on the feet and palms, pain, burning sensation, redness in affected site and secretions, and red or black colour of the particular area were reduced markedly.
Results of reducing symptoms such as itching, appearing of fissures, burning sensation and roughness were giving in the graphical way and calculated mean value of the response to Vipadikahara grita taila for each symptom was mentioned in “Y” axis and the time duration in weeks were mentioned in “X” axis.
Observed symptoms such as itching (by 90%; Figure 1) appearing of fissures (by 95.2%; Figure 2), pain (by 99.5%; Figure 3), burning sensation (by 98.7%; Figure 4), roughness (by 83.2%), eruption of papules (by 100%), redness (by 98.6%) and dark shades (by 83.4%) were reduced significantly in treated group than that of control group [itching (by 12.5%; Figure 1) appearing of fissures (by 15.6%; Figure 2), pain (by 19.2%; Figure 3), burning sensation (by 11%; Figure 4), roughness (by 30.3%), eruption of papules (by 38.1%), redness (by 21.4%) and dark shades (by 16.0%)].
Mean score of the length, width, depth of the ulcers and number of ulcers in the area of the lesions were significantly reduced by 91.9%, 94.8%, 91.9% and 90.1% respectively. In control group it was decreased by 19.6% in length, 12.7% in width, 36.4% in depth of the ulcers and 29.9% in number of ulcers in the area of the lesions. Hence, it is very clear that the symptoms of Vipadika Kushtha was significantly reduced by the application of Vipadikahara grita taila and it was found statistically significant at the level of P < 0. 01.
Overall result of individual groups showed that complete remission in treated group is zero, because though the patients got 100% relief from main symptoms (Figure 4), symptoms such as roughness, skin colour change and sometimes, few tiny bursts remain in the feet or palms. Hence, they categorized under the marked improved category. Accordingly, 72% (36 patients) showed marked improvement. Eighteen percent (09 patients) improved with 30% relief with unchanging the symptoms such as Itching, Roughness and black color change. Ten percent (05 patients) become unchanged.
In Control group, complete remission is zero, while 08% (04 patients) were come under improved category. They got more than 76% relief in the signs and symptoms of Vipadika skin disease. Six percent (03 patients) is moderately improved and they got between 51-75% relief in the signs and symptoms. Eighty six percent (43 patients) were unchanged.
Wound healing is a normal biological process in the human body. Many factors can adversely affect this process and lead to improper and impaired wound healing. Medicinal plants are important sources of new chemical substances that have beneficial therapeutic effects. Recently, there has been a growing interest in phytochemicals, which are plant-based products and traditional therapies, potential applications of topical phytochemicals for the enhancement of both acute and chronic wound healing in both developing and developed countries.
It was very clear that application of Vipadikahara grita taila helped to cure this skin lesion by absorption through the skin. According to available literature [14], 28% of the oil will be absorbed to the skin after remain on skin for some times. The selection of an optimum base for the topical preparation is extremely essential in Ayurveda as it provides easier access to the active principles of the drugs up to the deepest stratum of the skin. Ghee, sesame oil and cow’s milk containing in the Vipadikahara grita taila are assisting for this oily purpose. Absorption of substances through the skin depends duration of contact and on solubility of medication. In the clinical study, Vipadikahara grita taila was applied morning and evening after cleansing the wounds. Therefore, it remains several hours in the skin. These factors helped to permeate the active principles of the drug up to the deepest stratum of the skin. In addition, sesame oil is a source of vitamin A and E and they are good antioxidants. Antioxidants give protection against oxidative damage and promote healing [15].
Plant-based products have been used to treat wounds for centuries worldwide. Recently, fascinating new evidence has emerged to highlight the mechanisms of some of these traditional therapies. The most common mechanisms behind phytochemical-mediated enhanced wound healing are their antioxidant, anti-inflammatory, and anti-microbial effects [16]. Due to the hot extraction technique used to extract the ingredients when preparing the oil, most of the chemical compounds have been extracted into the oil. Therefore, it possesses high medicinal value though it contains less number of medicinal plants. Medicinal plants have bioactive compounds, which used for curing of various human diseases and play an important role in healing [17]. Screening of four medicinal plants of Vipadikahara grita taila it was clearly reveals that they contain phyto-constituents such as saponins, steroid glycosides and coumarins In addition, phenolic compounds and tannins are rich in R. cordifolia and L. reticulata. Alkaloids are present in B. aristata and R. cordifolia and flavanoids in R. cordifolia [18-21].
The most important bioactive compounds of the medicinal plants are alkaloids, flavanoids and phenolic compounds [21]. Natural antioxidants mainly come from plants are in the form of phenolic compounds such as flavonoids, phenolic acids, etc [22]. Phenolic compounds possess biological properties such as antiaging, anti-carcinogenic, anti-inflammatory, anti atherosclerosis, cardiovascular protection and improvement of endothelial function, as well as cell proliferation activities [23]. Phenolic compounds contain in the oil help to heal wounds in many ways such as analgesics, anti-inflammatory and antimicrobial activities. The alkaloids contained in plants are used in medicine as anesthetic agents [24]. Tannins with its protein precipitating and vasoconstriction effect [25], are known to hasten the healing of wounds, and inflamed mucous membranes [26]. The plant extracts contain saponins, which are known to produce inhibitory effect on inflammation [27]. The process of inflammation mediated by neutrophils and macrophages leading to the destruction of foreign debris and microorganisms results in the production of radical oxygen species [28].
Flavonoids are hydroxylated phenolic substances known to be synthesized by plants in response to microbial infection and they have been found to exert antimicrobial activity against a wide array of microorganisms in vitro [29]. Interestingly, Vipadikahara grita taila showed potent antibacterial activity against Streptococcus pyogenes by agar well diffusion method [30]. Therefore, Vipadikahara grita taila can be used for infected skin ailments (especially for Streptococcus pyogenes) as an external application other than that of curing the fissures in Vipadika.
Moist wound healing from Ayurveda is more than mere moisture retention. Since emollients are used, they permeate easily through the skin and deeper fascia; they are full of nutrients and provide the right pH (acidic) for healing [15]. Active ingredients of the absorbed medicines must cross the epidermis, glands or hair follicles when it penetrates the skin. Sweat glands and hair follicles make up about 0.1% to 1.0% of the total skin surface [31]. Though small amounts of chemicals may enter the body rapidly through the glands or hair follicles, they are primarily absorbed through the epidermis. Chemicals must pass through the seven cell layers of epidermis before entering the dermis where they can enter the blood stream or lymph and circulate to other areas of the body [14]. Accordingly, Active ingredients of the absorbed medicines in medicated oil cross the epidermis and glands to penetrate the skin.
When considering on Ayurveda aspect of the oil, ghee has the properties of Sanskaranuvartini (which assimilates the properties of other drugs during drug development) according to Caraka samhita Sutra chapter [31]. Hence, it is an ideal base for wound healing applications. Further, ghee contains property of yogavahi: a catalytic agent that carries the medicinal properties of herbs into the seven tissues of the body. Ghee has opposite qualities and thus pacifying effects to the light, dry and rough qualities of Vata dosha. Ghee pacifies Pitta and Vata in moderation for Kapha. Vipadikahara grita taila contain 77.8% sweet (Madhura) and 55.5% oily (Snigdha) properties. Further, it has 55.6% cold potency (Shita Virya), Madhura vipaka (end result effect is sweet) and 88.9% alleviate Vata and Kapha properties with 66.7% alleviate Pitta properties. Alleviation of Vata is mainly done by the oily property of two oils (ghee and the sesame) and cow’s milk. These two oils specially contain the properties of alleviation of Pitta and Vata humors. Further, resin of Shorea robusta Geartn has such as wound cleansing, wound healing and blood clotting properties, which help to cure Vipadika skin disease.
According to the statistical analysis, treated group showed significantly greater wound healing activity compared to the control group by reducing all symptoms. Additionally, the control group showed marginal improvement with reducing roughness, pain and eruption of papules. It is understood that the observed inhibition is due to the base formulation of the oil. Therefore, it is very clear that the properties of medicinal plants and the other ingredients of the oil support the wound healing mechanisms.
Most of the patients in treated group had shown stable response during the follow- up. Few of the patients (four patients) showed re-occurrence of the symptoms after treatment. This may be due to improper diet and regimen which might have followed by the patients. Hence, when comparing two groups, treated group has shown effect that is more potent over all during treatment, after treatment and after follow up.
Normally, both internal and external medicines together have promising activity to achieve the complete cure for Vipadika skin disease. According to the studies carried out in Ayurveda, very few had been done relate to Vipadika skin disease and all are followed the line of treatment with multiple medicine collectively. However, in this research only the medicated oil was tested against Vipadika skin disease and the findings have shown the effect of one external medicine as a complete treatment for Vipadika skin disease. Hence, Vipadikahara grita taila has given new positive results in Ayurveda aspect and as well as in scientific aspect.
Present study had proven that, Vipadikahara grita taila could be used externally as an effective medicated oil to manage a type of Kshudra Kushtha called Vipadika.
National Centre for Advanced Studies for Humanities and Social Sciences, Ward place, Colombo 7, Sri Lanka, is acknowledged for financial assistance.
The data used to support the findings of this study are available from the corresponding author upon request via sujathahgsp@yahoo. com or Ph.D thesis [Hewageegana, H.G.S.P. (2015)]. A study of skin diseases: Ksudra kustha depicted in Sanskrit original sources with special reference to Vipadika and its management. Ph.D. Thesis, University of Kelaniya] which deposited at University of Kelaniya, Sri Lanka.

![]()

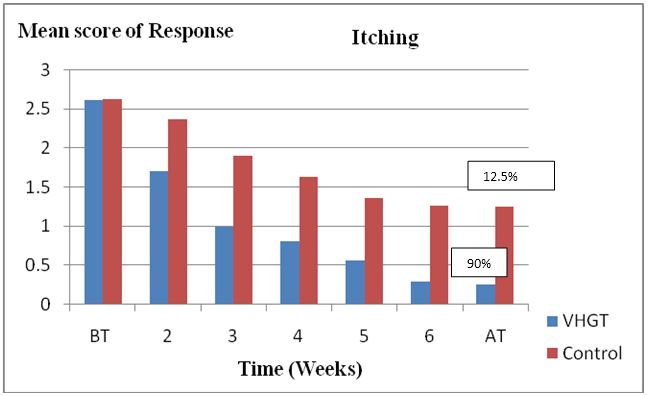 |
| Figure 1: Effect of Vipadikahara Grita Taila (90% Reduction) and Control (12.55% Reduction) on Itching of the Lesion before Treatment (BT) and After Treatment (AT). The Results are Compared to Control and Reduction of the Itching of the Fissure was Statistically Significant at the Level of P < 0.01. VHGT- Vipadikahara Grita Taila |
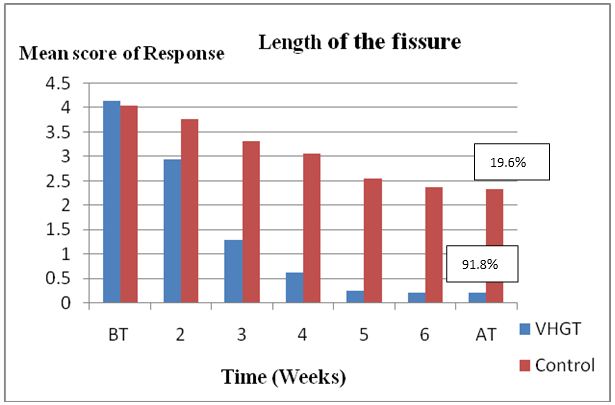 |
| Figure 2: Effect of Vipadikahara Ghrita Taila (90% Reduction) and Control (12.55% Reduction) on Length of the Fissure before Treatment (BT) and After Treatment (AT). The Results are Compared to Control and Reduction of the Length of the Fissure was Statistically Significant at the Level of P < 0.01. VHGT- Vipadikahara Grita Taila |
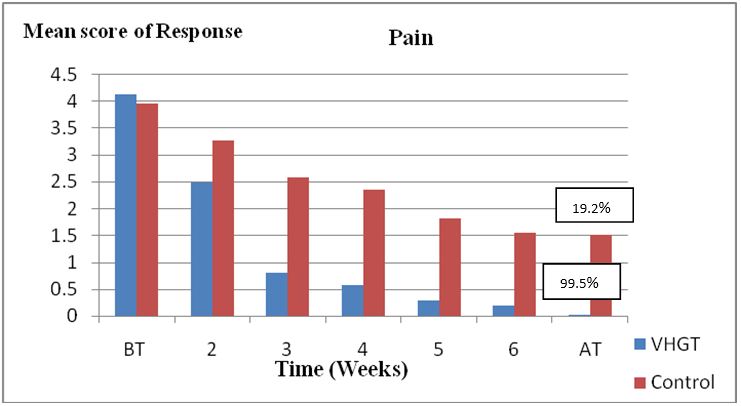 |
| Figure 3: Effect of Vipadikahara Grita Taila and Control on Pain of the Lesion before Treatment (BT) and After Treatment (AT). The Results are Compared to Control and Reduction of the Pain of the Fissures was Statistically Significant at the Level of P < 0.01. VHGT- Vipadikahara Grita Taila |
 |
| Figure 4: Symptoms of Vipadika Kushtha Was Reduced After 06 Weeks of Treatment with Vipadikahara Grita Taila |
Parameters |
VHGT |
Control |
||
Before Treatment |
After Treatment |
Before Treatment |
After Treatment |
|
W B C Count (cumm) |
7100 ± 240 |
6900 ± 250 |
6600 ± 250 |
6700 ± 260 |
R BC Count (x 10 6) cumm |
4.97 ± 0.23 |
5.03± 0.31 |
5.04±0.28 |
5.11±0.57 |
F BS Levels (mg/dL) |
94.92±1.79 |
94.76±1.89 |
91.09 ±1.36 |
91.00±1.21 |
Blood Urea Levels (mg/dL) |
19.86 ± 1.64 |
20.32 ± 1.84 |
21.33 ± 1.06 |
21.35 ± 1.09 |
Specific Gravity of Urine |
1.020 ± 0.18 |
1.021 ± 0.21 |
1.026 ± 0.18 |
1.023 ± 0.27 |




































