Open Access
Research Article
Max Screen
Copyright: © 2024 Redwan Shifa. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:Erectile dysfunction in diabetic males is considerably high, but it is often underdiagnosed and under-managed. Identifying the status and risk factors of erectile dysfunction is important in sexual quality of life and maintaining partner relationships.
Objectives:To assess erectile dysfunction and associated factors among adult diabetic males attending Jimma Medical Center from May 15 to June 15, 2023.
Methods:An institution-based cross-sectional study was conducted among 421 male diabetic patients at a follow-up clinic in Jimma Medical Center from May 15 to June 15, 2023, and participants were required by the Consecutive sampling method. The participants were interviewed using structured questionnaires. Binary logistic regression analysis was performed to analyze the association between a dependent variable and an independent variable, and variables with a p-value less than or equal to 0.05 were considered statistically significant. The strength of association was measured using an odds ratio at a 95% confidence level. Finally, the result was presented by using texts, tables, and graphs.
Result:The prevalence of erectile dysfunction in this study was 354 (89.2%). The study found that age had an adjusted odds ratio of 2.75 (95% CI: 1.378-5.498; p 0.004), duration of diabetes had an adjusted odds ratio of 2.5 (95% CI: 1.261-4.961; p 0.009), type of diabetes had an adjusted odds ratio of 2.2 (95% CI: 1.107-4.455; p 0.025), and chewing khat had an adjusted odds ratio of 5.83 (95% CI: 1.911-17.772; p 0.002) with a positive significant association with erectile dysfunction.
Conclusions and Recommendation:The findings of this study suggest that age, type two Diabetic Mellitius, duration of Diabetic Mellitius above years, and chewing khat were statistically significant with erectile dysfunction. Healthcare providers should inform diabetes patients about the risk factors of erectile dysfunction and Screening for erectile dysfunction for males with Diabetic Mellitius who are aged above 40 years, as early detection, treatment, and possibly prevention should be given.
Keywords: Erectile dysfunction; Diabetes mellitus; Jimma Medical Center
Diabetes mellitus is a long-term health condition affecting various organs, with erectile dysfunction being a common complication, affecting male diabetic individuals' quality of life by preventing successful sexual activity [1, 2]. Erection is a complex process involving hormonal, vascular, neural, and psychological factors, occurring in four stages: desire, erection, ejaculation, and detumescence, with both initiation and maintenance phases [3].
Erectile dysfunction can be caused by organic or psychogenic factors, possibly linked to Diabetic Mellitus. Organic causes may include vascular issues, trauma, neurological conditions, endocrine imbalances, or drug side effects [4]. Erectile dysfunction in diabetic males requires a comprehensive approach, including modifiable risk factors, lifestyle changes, and phosphodiesterase 5 inhibitors, due to its multifactorial nature [5].
Erectile dysfunction significantly affects a man's quality of life, affecting sexual performance, anxiety, depression, relationships, self-esteem, and engagement in social and work-related activities, leading to psychological and social consequences [6, 7].
Research on diabetes complications has mainly focused on severe ones, but erectile dysfunction, a common overlooked issue, is being increasingly recognized as an early warning sign for cardiovascular disease in individuals with Diabetes Mellitus [8].
Erectile dysfunction is more prevalent in diabetic men than non-diabetic men, with over 63% prevalence in Sri Lanka [9], 69% in India(10), 87% in Saudi Arabia [11], 81% in Sudan [12], and 79% in the Democratic Republic of Congo [13].
In Ethiopia, the overall prevalence of erectile dysfunction among patients with Diabetic Mellitius was 54.3% [14]. A study done in northwestern Tigray prevalence of erectile dysfunction was 69.9% [15], 53% in Gondar [16], 86% in Bahir Dar [17], and 60.4% in Jimma [18].
Erectile dysfunction in males with Diabetic Mellitus increases with age, duration, metabolic control, and other complications. Over 45, prevalence increases, leading to decreased self-esteem. Interestingly, primary care physicians often fail to address this issue [16].
Sexual disorders in Ethiopia are frequently overlooked and underreported, with many healthcare professionals neglecting aggressive intervention strategies due to societal taboos and societal pressures to report erectile dysfunction [19].
Erectile dysfunction may lead to serious psychosocial and clinical outcomes such as decreased quality of life and depression [20–22]. Despite limited research on its relationship with sexual quality of life,this research aims to evaluate erectile dysfunction and its related factors in male diabetics receiving care at a diabetic clinic in Jimma Medical Center, Oromia, South West Ethiopia, 2023.
This study was conducted at a public hospital in Jimma town, Oromia, Ethiopia from May 15 to June 15, 2023. Jimma Medical Center is one of the oldest public hospitals in Jimma town and it is the only teaching and referral hospital in the southwestern part of the country. It provides services for approximately 19,000 inpatients, 160,000 outpatient attendances, 5,000 delivery, and 11,000 emergency cases annually. It has a bed capacity of 800 and an estimated total number of 14,000 adult patients admitted annually. The hospital has 1,600 staff members, 23 service delivery units, 698 Staff nurses, 125 pharmacy staff, and different working units like medical, surgical, maternity, gynecology, oncology, ophthalmology, psychiatry, and the like. Approximately, 19,000 patients attend the follow-up clinic and on average 421 male DM Patients visit the follow-up clinic every month [23].
An institutional cross-sectional study design was used.
All diabetic patients who have follow-ups at the chronic follow-up clinic at Jimma Medical Center
All male patients with diabetes attended the chronic follow-up clinic at Jimma Medical Center during the study period.
Adult males with Diabetic Mellitius and age group ≥18 years who are on follow-up at the chronic follow-up clinic at Jimma Medical Center during the study period and patients who voluntarily participated in the study.
Mentally impaired patients, seriously ill, patients with known secondary erectile dysfunction from genetic or surgical causes, and those who had on follow-up of less than one year were excluded from the study.
All male diabetic patients who were on follow-up at the chronic follow-up clinic of Jimma Medical Center were included in the study, which comprised 421 male diabetic patients and was conducted using a Consecutive sampling method.
The study participants who were on follow-up at the chronic follow-up clinic at Jimma Medical Center from May 15 to June 15, 2023 was consecutively recruited.
Erectile dysfunction
Socio-demographic factors (includes Age, Marital status, Educational status, Occupational status, Monthly income, Resident), Lifestyle behavior(includes History of alcohol, Status of physical exercise, History of smoking, Chewing chat. BMI), Clinical factors(includes Type of DM, Duration of the DM, Fast blood glucose level (FBS), DM-related microvascular complications, Drugs for the DM, Co-morbid (Hypertension, CKD, IHD), and Sexual quality of life which includes Relationship with partner, Satisfaction with the treatment of ED, and psychological impacts.
Erectile dysfunction(ED):The presence of erectile dysfunction was established by using the International Index of erectile function (IIEF-5). Individuals who scored 1–21 out of 25 points were reported as having ED [24]. Individuals who scored 1–7out of 25 points were reported as having Severe ED [25], Individuals who scored 8–11 out of 25 points were reported as having Moderate ED [25], Individuals who scored 12–16 out of 25 points were reported as having mild-moderate ED [25], and Individuals who scored 17–21 out of 25 points were reported as having MildED [25].
Regular exercises:Patients with diabetes who participated in at least 30 min of physical activity daily or participated in a specific exercise session were considered to have adequate physical activity; otherwise, the patient was classified as having inadequate physical activity [26].
Co-morbid illness:Existence of additional chronic illnesses, including hypertension, cardiac disease, dyslipidemia, psychosis, renal disease, HIV, cancer, asthma, and multiple sclerosis [27].
Social drug use:The lifestyle of the patients was assessed during the patient interview. If the patients responded "Yes" to smoking cigarettes, drinking alcohol, and chewing khat, the patients were recorded as smokers, alcohol drinkers, and khat chewers, respectively [26].
Poor sexual quality of life:if the sum of the participant's score of SQOL item is < 50% which means less than or equal to 32 out of 64, the participants have good sexual quality of life [28].
Good sexual quality of life:if the sum of the participant's score of SQOL item is > 50 % which means greater than 32 out of 64, the participants have good sexual quality of life [28].
Interviewer-administered questionnaires adopted from different sources were used to collect the data. A validated questionnaire adopted from the 5-item version of the International Index of Erectile Function (IIEF-5) was used for erectile dysfunction. This multidimensional tool evaluates five aspects of sexual function such as erectile function, orgasm, desire for sex, satisfaction after intercourse, and overall satisfaction. Each aspect was assessed by a five-point Likert scale and the scores ranged from 0 to 25 was used [6, 29]. A structured questionnaire was used to collect relevant socio-demographic, lifestyle factors and clinical information such as age, marital status, occupational status, monthly income, educational status, Body Mass Index (BMI), smoking status, chewing chat, type of DM, the status of glycemic control, comorbidity, and duration of DM will major measure of ED. Sexual-related quality of life questions and treatment satisfaction were used for assessing the sexual quality of life among ED in diabetic patients, the instrument consists of 16 items, 10 of which deal with dimensions of sexual QOL that can be summed to a sexual QOL scale measure. The remaining six items comprise a scale measuring satisfaction with treatment dimensions [20].
Two male BSc nurse were selected from Shanen Gibe Hospital, considering their previous experience in data collection. Data was collected in face-to-face interviews using a structured and translated local-language questionnaire and the patient’s clinical-related factors were extracted from a patient card using a chart extraction checklist when needed.
The questionnaire prepared in English was translated to the local language (both Afaan Oromo and Amharic) by multilingual translators. To ensure the quality of data questionnaires were pre-tested on 5% of the sample size (20 study participants) in Limmu Genet Hospital to check data for response accuracy and to identify possible obstacles that might be encountered during data collection as well as to estimate the time needed to complete the item. Based on the feedback given some editorial modifications, such as correcting the spelling of the questionnaire, it was eventually integrated into the final tool.
One day of training was given to data collectors to ensure that all the data collectors had a common understanding of the study instrument and should follow the same interview procedures. Continuous follow-ups were made by the principal investigator throughout the data collection period. Daily reviewing or checking of all the completed questionnaires was made by the principal investigator to ensure completeness and consistency of the collected data. Privacy was respected. All the questionnaires are unnamed and participants were interviewed alone in a private room.
Data were edited, coded, and entered by Epidata version 3.1 and were exported to SPSS (version 25) for analysis. The data analysis started from a basic description to the identification of potential factors associated with erectile dysfunction. Bivariable and multivariable logistic regression were used to identify the relationship between erectile dysfunction and various factors. The assumptions of the logistic regression model Hosmer-Lemeshow goodness of fit statistics were checked and satisfied. Multivariable logistic regression was used to identify potential confounding variables. Multicollinearity among independent variables was checked using tolerance and variance inflation factors. Normality for independent variables was checked using Shapiro Wilk. Descriptive summaries were computed as simple frequencies, mean, median, and standard deviations.
All explanatory variables which resulted in p < 0.25 with the outcome variable in the bivariable were entered into a multivariable logistic regression model to identify factors associated with erectile dysfunction. P-value < 0.05 was considered statistically significant and the adjusted odds ratio with a 95% confidence interval was used to declare the association. Finally, the result was presented by using texts, tables, and graphs.
Before data collection, ethical clearance and approval to conduct the study were obtained from the Institutional Review Board of Jimma University, Institute of Health with ethical review code of JUIH/IRB/390/23. Then a letter was secured from the university to gain support for the study. Before administering the questionnaires, the aims and objectives of the study were explained to the participants and informed written consent was obtained from the study participants after explaining the objective of the study. They had been told that participation was voluntary confidentiality and privacy was ensured throughout the execution of the study, as participants were not required to disclose personal information on the questionnaire and were interviewed alone in a separate room.
This study findings highlight sociodemographic charectersitc, Lifestyle characteristics ,clinical characteristics,its prevalence and associated factor with erectile dysfunction of diabetic males attending Jimma Medical Center, Sociodemographic characteristics of diabetic males attending JMC.
Out of the total of 404 diabetic patients planned to be interviewed 397 of them were interviewed giving a response rate of 98.27%. The mean age of the respondents was 47.43 (±SD=13.183) years with a range of 18-76 years. The majority of respondents 363 (91.4 %) were married and 118 (29.7%) of them completed primary school. Around, 94 (23.7%) were farmers, and 229(57.7%) were from the rural. The mean monthly income of participants was 4200.45+2704.383 SD Ethiopian Birr and 164 (41.3%) of participants were above 5000 ETB (Table 1).
According to this study, 311 (78.3%) of the participants did not consume alcohol, 369 (92.2%) of the participants did not smoke cigarettes, 266 (67.0%) of the participants chewed khat and only 112 (28.2%) of the participant engaged in a regular physical exercise respectively. (Table 2)
In this study about 335 (84.4%) of the participants had type II DM and 23(81.4%) of them used oral hypoglycemic medication. Additionally 311 (78.3%) of the participants lived with DM 5 and above. Furthermore, 370 (93.2%) of the participants were adherent to their DM drug. The study also found that 233 (58.7%) of the participants had normal normal fasting blood sugar levels (< 126mg/dl). Moreover, 265(66.8%) of the participants were within the normal range for blood pressure, and 227 (57.2%) of participants had poor quality of sexual life (Table 3).
In this study out of 404 studies, participant prevalence of ED was 354 (89%) which is very high (figure-1). Severity of erectile dysfunction categorized as 153(38.5%) had mild-moderate ED, 82(20.7%) of the participant had mild ED, 71(17.9%) participant had moderate ED and 48(12.1%) was had severe ED (Figure-2).
The bivariate logistic analysis of socio-demographic, lifestyle, and clinical characteristics of participants with ED and candidates for this model were age, residence, type of hypoglycemic drug, marital status, blood pressure, weight, SQL, khat, BMI,Type of DM, and duration of DM.
The study finding shows that the odds of having erectile dysfunction among diabetic patients were 2.75 times more likely higher in participants with ages above 40 years than those ages between 18 and 40 years.
According to the study, the odds of having erectile dysfunction among diabetic patients were 2.50 times more likely higher in participants with a duration of diabetes > 5 years than those with diabetes with a duration of < 5 years. The study finding suggests that the odds of having erectile dysfunction among diabetic patients were 2.22 times more likely higher in participants with Type II diabetics than that of Type I diabetics. The study found that the odds of having erectile dysfunction among diabetic patients were 5.83 times more likely higher in participants with chewing khat than those who did not chew chat (Table 4).
The study found that a majority of study participants experienced erectile dysfunction. Around 89.2% of study participants had erectile dysfunction. The severity of the dysfunction varied based on factors such as age, khat chewing, type of DM, and duration of DM. This indicates that the prevalence of erectile dysfunction among diabetic patients was high. This leads to negative consequences such as loss of self-esteem, anxiety, depression, separation from sexual partners, and isolation.
The finding of this study is in line with the study done at Kinshasa University in the Democratic Republic of the Congo, 87.5% [13]. But higher than the study conducted in Mettu at 82.1% [26], Sudan at 81.1% [12], Egypt at 80% [30], Hawasa at 72.2% [6], and northwest Amhara at 69.5% [27]. The prevalence of erectile dysfunction among diabetic patients seems to vary across different regions and studies. There could be several factors contributing to this discrepancy, such as differences in the study area, which could be due to socio-cultural differences, variation in sample size, study period, study method, lifestyle, and sociodemographic characteristics of the participants. Factors associated with erectile dysfunction are age above 40 years, duration of diabetes of above 5 years, chewing chat, and type II diabetes.
The study finding shows that the odds of having erectile dysfunction among diabetic patients were three times more likely higher in participants with ages above 40 years than those ages between 18 and 40 years. This is supported by a study done in the eastern part of Sudan, Tanzania, and Ethiopia, which showed that age was positively associated with ED [12, 13, 16]. As a person ages, their testosterone levels can decline, which could potentially decrease erectile function. Additionally, as age increases,the decline in vascular function, nerve conduction, and hormonal levels that are involved in erectile function could also be contributing factors.
The study results show that the odds of having erectile dysfunction among diabetic patients were three times more likely higher in participants with a duration of diabetes > 5 years than those with diabetes duration of < 5 years. This is supported by a study done in northwest Amhara, Gondar, which showed that the duration of diabetes was positively associated with ED [16, 27]. As a person's duration of diabetes increases, there is a possibility of damage to the nerves and blood vessels, moreover, as the duration of diabetes increases levels of oxidative stress which is when the body produces too many free radicals that can damage cells and tissue, including nerves and blood vessels which could lead to erectile dysfunction.
According to the study, the odds of having erectile dysfunction among diabetic patients were two times more likely higher in participants with Type II diabetics than those of Type I diabetics. This is supported by a study conducted in southwest Ethiopia and Mettu which showed that Type II diabetics were positively associated with ED [19, 26]. As a person with Type II diabetes, there is a higher likelihood of having cardiovascular risk factors such as hypertension and dyslipidemia, which can lead to erectile dysfunction. Moreover, due to insulin resistance, the body is unable to metabolize glucose effectively, leading to high blood sugar levels that can damage nerves and blood vessels over time. This damage can ultimately result in erectile dysfunction.
The study findings suggest that the odds of having erectile dysfunction among diabetic patients were six times more likely higher in participants with chewing khat than those who did not chew chat. This is contradicted by a study done in Yemen which showed that chewing khat was negatively associated with ED [32]. As a person who chews khat, there are psychoactive compounds present in it, including cathinone. These compounds have vasoconstrictive effects that may lead to developing erectile dysfunction. The discrepancies in the findings of different studies may be due to differences in the way khat is chewed, the amount of khat chewed, or the frequency of khat chewed. Additionally, the two studies were conducted in different countries and had different sample sizes, methodologies, and cultural differences. Therefore, it is difficult to make a direct comparison between the two studies. However, more research is needed to better understand the relationship between chewing khat and erectile dysfunction.
Moreover, due to the nature of the study design, information concerning the relationship between variables was provided in a short period. Since the study data was taken from a large sample of participants it increases the generalizability of the findings., the cause-and-effect relationship could not be established, and also the study site was in a tertiary center it's likely that the respondents had more complicated medical conditions than other sites. Furthermore, the study may be prone to social desirability bias due to sensitive questions related to sexual issues.
The findings of this study suggest that erectile dysfunction is a common problem among diabetic patients and age, type II DM, duration of DM > 5 years, and chewing khat were statistically significant. Healthcare providers should inform diabetes patients about the risk factors of ED and pay more attention to their sexual history to diagnose and manage ED more frequently. Screening for ED for males with DM who are aged above 40 years and have been living with DM for more than 5 years, as early detection, treatment, and possibly prevention can be achieved. In addition, patients should not chew khat to reduce the prevalence of ED.
Abbreviation: BMI: Body Mass Index; DM: Diabetes Mellitus; ED: Erectile Dysfunction; EDHS: Ethiopian Demographic Health Survey; IIEF: International Index of Erectile Function; JMC: Jimma Medical Center; MARD: Mild Age-Related Diabetes; MOD:Mild Obesity-Related Diabetes; SIRD: Severe Insulin-Resistant Diabetes; SQOL: Sexual Quality of Life; WHO: World Health Organization
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
The fund for this survey conducted was obtained from Jimma University, but The authors have no financial support for the research, authorship, and/or publication of this article.
The study protocol was approved by the Research Ethics Committee of Jimma Medical Center. No study procedures were performed before obtaining all participants’ written and informed consent.
Reduwn Shifa: Data curation, Formal analysis, Methodology, Resources, Software, Validation, Writing original draft, review, and editing. Wadu Walancho: Investigation, Supervision, Validation, Visualization, Writing review & editing. Sadik Abdulwehab: Conceptualization, dta curation,Validation, Visualization, Writing review & editing. Fikadu Belcha: Conceptualization, Supervision, Validation, Visualization, Writing review & editing Finally, All authors read & approved the manuscript for submission.
We would like to acknowledge Jimma University for funding the survey cost. We are also thankful to our study subjects for their time and valuable information.
Not applicable
All concerned bodies involved in this manuscript either financially or technically were appraised. So we declare that we are accountable for any conflict of interest if any

![]()

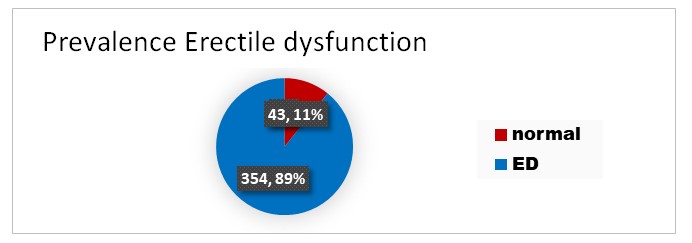 |
| Figure 1: prevalence of erectile dysfunction among diabetic patients attending JMC |
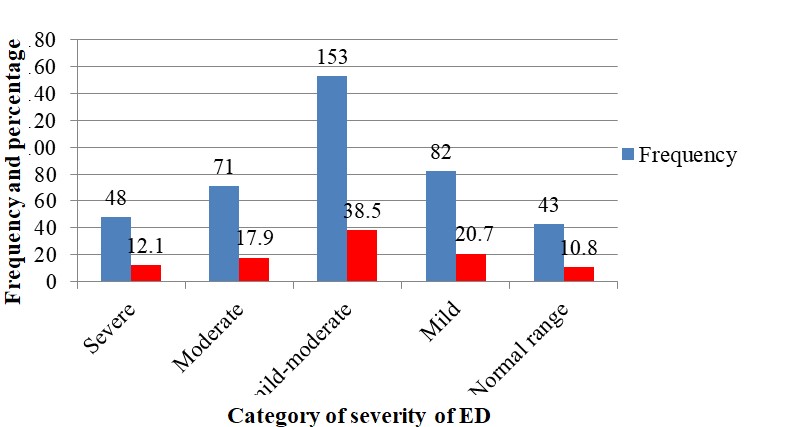 |
| Figure 2: Severity of erectile dysfunction among diabetic patients attending JMC |
Variable |
Category |
Frequency(N) |
Percent (%) |
Age in years |
18-24 |
50 |
12.6 |
25-35 |
49 |
12.3 |
|
36-45 |
75 |
18.9 |
|
46-55 |
96 |
24.2 |
|
56-65 |
83 |
20.9 |
|
>65 |
44 |
11.1 |
|
Marital status |
Single |
20 |
5.1 |
Married |
363 |
91.4 |
|
Other |
14 |
3.5 |
|
Educational status |
Illiterate |
42 |
10.6 |
read and write |
66 |
16.6 |
|
primary education |
118 |
29.7 |
|
high school |
107 |
27.0 |
|
College and above |
64 |
16.1 |
|
Occupational status |
Unemployed |
36 |
9.0 |
Daily laborer |
44 |
11.1 |
|
Merchant |
56 |
14.1 |
|
Government employee |
63 |
15.9 |
|
Private/NGO |
75 |
18.9 |
|
Farmer |
94 |
23.7 |
|
Other |
29 |
7.3 |
|
Residency |
Urban |
168 |
42.3 |
Rural |
229 |
57.7 |
|
Monthly income in ETB |
<1500 |
86 |
21.7 |
1500-5000 |
147 |
37.0 |
|
>5000 |
164 |
41.3 |
Variables |
Frequency (N) |
Percent (%) |
|
Alcohol |
Yes |
86 |
21.7 |
No |
311 |
78.3 |
|
Smoking |
Yes |
28 |
7.1 |
No |
369 |
92.9 |
|
Khat |
Yes |
131 |
33.0 |
No |
266 |
67.0 |
|
Regular exercise |
Yes |
112 |
28.2 |
No |
285 |
71.8 |
|
Variables |
Frequency (N) |
Presents (%) |
|
Type of diabetes |
T1DM |
60 |
15.1 |
T2DM |
337 |
84.9 |
|
Type of hypoglycemic drug used |
Oral |
329 |
82.9 |
Injectable |
59 |
14.8 |
|
Both |
9 |
2.3 |
|
Duration of the DM |
Below 5 years |
86 |
21.7 |
5 and above |
311 |
78.3 |
|
Glucose level (FBS) |
Below 126 |
233 |
58.7 |
126 and above |
164 |
41.3 |
|
Blood pressure |
Normal |
265 |
66.8 |
Pre HTN |
89 |
22.4 |
|
Stage I HTN |
35 |
8.8 |
|
Stage II HTN |
8 |
2.0 |
|
Adherence to DM drugs |
Yes |
370 |
93.2 |
No |
27 |
6.8 |
|
Reason does not adhere |
Drug shortage |
22 |
5.5 |
Affordability |
4 |
1.0 |
|
Poor communication with Health workers |
15 |
3.8 |
|
Negligence |
2 |
0.5 |
|
Comorbid |
Hypertension |
70 |
17.6 |
CHF/IHD |
14 |
3.5 |
|
Chronic kidney disease |
1 |
0.3 |
|
Chronic liver disease |
5 |
1.3 |
|
Others |
2 |
0.6 |
|
Treatment for ED (n= 354) |
Yes |
34 |
9.6 |
No |
362 |
91.2 |
|
Sexual quality of life |
Poor |
227 |
57.2 |
Good |
170 |
42.8 |
|
Variables |
Category |
ED |
COR |
AOR 95% CI |
P-Value |
|||||
YES |
NO |
|
||||||||
Age |
18-40 |
126(82.4%) |
27(17.6%) |
1 |
1 |
|
||||
>40 |
228(93.4%) |
16(6.6%) |
3.054(1.585-5.882) |
2.753 (1.378-5.498) |
0.004 |
|||||
Type of DM |
Type I |
86(81.9%) |
19(18.1%) |
1 |
1 |
|
||||
Type II |
268(91.8%) |
24(8.2%) |
2.467(1.289-4721) |
2.220 (1.107-4.455) |
0.025 |
|||||
Duration of DM |
<5 years |
104(80.6%) |
25(19.4%) |
1 |
1 |
|
||||
>5years |
250(93.3%) |
18(6.7%) |
3.339(1.747-6.380) |
2.501 (1.261-4.961) |
0.009 |
|||||
Khat |
Yes |
154(97.5%) |
4(2.5%) |
7.507(2.627-21.46) |
5.828(1.911-17.772) |
0.002 |
||||
No |
200(83.7%) |
39(16.3%) |
1 |
1 |
|
|||||




































