Open Access
Research Article
Max Screen
ISSN: 2394-6504
Copyright: © 2021 Kojuri J. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:Cardiovascular disease (CVD) is one of the most common causes of mortality and morbidity worldwide. Coronary artery disease (CAD) is the most common form of CVD. To prevent CAD we need to assess the risk of future CAD in all patients referred for cardiovascular care, but each of the several available systems for risk assessment has its own limitations. This study was designed to determine whether vitamin D deficiency is a potential risk factor for CAD.
Method:Between 2018 and 2020 we conducted a large cross-sectional population-based study of 4526 patients in Shiraz, Iran. All patients underwent selective coronary angiography via a radial artery approach by an expert interventional cardiologist. Serum levels of 25-hydroxy vitamin D and high-sensitivity C-reactive protein (hs-CRP) were measured in all patients.
Results:Mean vitamin D level was lower in patients with significant CAD (27.2±14.8) than in patients with non-significant CAD (29.5±14.8). The difference was statistically significant (p< 0.001). There was no correlation between vitamin D and hsCRP levels (rho=0.04, p=0.204). Vitamin D deficiency was more frequent in men (2499, 70.4%) than women (1486, 58.6%). This difference was statistically significant (p< 0.001).
Conclusion:Our findings show a significant association between vitamin D deficiency and the prevalence of CAD independent of hs-CRP level, and suggest a correlation between vitamin D levels and the severity of CAD. In addition, mean 25-hydroxy vitamin D level was lower in men than in women.(Clinical trial.gov registration number: NCT04651101).
Keywords: Coronary Artery Disease; Vitamin D Deficiency
Vitamin D is a steroid fat-soluble vitamin with important roles in bone metabolism and metabolic, cardiovascular and dermatologic tissues [1]. Vitamin D receptors have been detected in myocytes, cardiomyocytes, pancreatic beta cells, vascular endothelial cells, neurons, immune cells, and osteoblasts [2]. It is known that vitamin D plays favorable roles in the immune-inflammatory process of atherosclerosis, and also has positive effects in conditions that can accelerate atherosclerosis such as dyslipidemia, insulin resistance and the complications of hypertension. Vitamin D needs two hydroxylation steps to become active. Initial hydroxylation occurs in the liver and forms 25-hydroxy vitamin D (25 (OH)D). The second hydroxylation occurs mostly in the kidneys, and forms 1,25-hydroxy vitamin D. The main active form of vitamin D3 is 1,25-(OH)2D3, but as an indicator of vitamin D status at the whole-body level, 25-hydroxy vitamin D is used [3].
Recent studies have shown a close relationship between CAD and vitamin D deficiency [4-6]. Moreover, low serum levels of 25-hydroxy vitamin D can be an absolute risk marker for cardiovascular events and mortality [7]. However, some studies have disputed this connection [8,9]. Jarrah et al., for example, found no significant association between vitamin D abnormalities and the incidence of CAD [10].
High-sensitivity C-reactive protein (hs-CRP) is known to be an acute-phase reactant inflammatory marker often present in atherosclerotic lesions [11]. High levels of hs-CRP are associated with an increased risk of CAD because this protein contributes to atherogenesis, plaque formation and plaque rupture [12].
Because of the controversial nature of the association between vitamin D levels and the occurrence of CAD, this study was designed to determine whether serum 25-hydroxy vitamin D level was associated with CAD in large group of patients, and to determine whether vitamin D deficiency may be a risk factor for CAD.
The clinical data for this cross‐sectional study in Shiraz, Iran, were collected from patients referred to Professor Kojuri Cardiovascular Clinic in Shiraz, Iran (Email: kojurij@yahoo.com, webpage: http://kojuriclinic.com/) from March 2018 to March 2020. The inclusion criterion was new symptomatic patients referred to Professor Kojuri Cardiovascular Clinic during the study period and were suspicious to have coronary artery disease based on non-invasive tests . The exclusion criteria were serum level of 25-hydroxy vitamin D3 higher than 100 ng/mL, parathyroid disorders, end-stage renal disease, and paraneoplastic syndromes. Patients whose serum level of hs-CRP was higher than 10 mg/L were also excluded.
Complete history was noted and the findings on physical examination were recorded for all patients, and risk factors such as hypertension, diabetes mellitus, age and gender were considered. In all patients 25-hydroxy vitamin D3 level and blood pressure were recorded, and electrocardiographic tracings were obtained. The dependent variable was the prevalence of CAD, the independent variable was vitamin D deficiency, and intervening factors were age, gender, hypertension, diabetes mellitus and level of hs-CRP.
All patients underwent selective coronary angiography via a radial artery approach by an expert interventional cardiologist. Angiography videos were reviewed by a team of expert cardiologists; based on the results, significant CAD is defined as >50% stenosis of the left main stem or >70% stenosis in a major coronary vessels. Diabetes was defined according to ADA 2018 criteria [13], and hypertension was defined according to ACC/AHA 2017 criteria [14]. Serum level of 25-hydroxy vitamin D on the patient’s first visit was used as an index of vitamin D level. Vitamin D deficiency was defined as a serum level of 25-hydroxy vitamin D less than 30 ng/mL, and sufficiency was defined as a serum level of 25-hydroxy vitamin D greater than 30 ng/mL [15].
For statistical analyses we used IBM SPSS software version 25. Independent-sample t tests and one-way ANOVA were used for parametric variables. The Mann-Whitney U test and Kruskal-Wallis test were used for nonparametric data. We used Pearson correlation for continuous variables. Values of p < 0.05 were considered significant.
All patients were informed about the details of this research, and provided their written informed consent. Patients who declined to participate in the study were excluded. The protocol was approved by the Ethics Committee of Shiraz University of Medical Sciences under code IR.SUMS.MED.REC.1398.246.
During the study period 4526 new patients were referred to Professor Kojuri Cardiovascular Clinic. 292 patients were excluded based on the exclusion criteria, and vitamin D was measured in the remaining 4234 patients (2490 men [58.8%] and 1744 women [41.2%]). Mean age of the patients in this study was 64.89 ±10.7 years (Table 1).
All 4234 patients underwent coronary angiography. According to the results, 1053 patients (24.9%) were considered to have nonsignificant CAD, and the remaining 3181 patients (75.1%) were considered to have significant CAD.
Mean vitamin D level was 27.78±14.69 ng/mL. Vitamin D deficiency was found in 2755 patients (65.1%), and sufficiency was found in 1479 patients (34.9%) (Table 2).
Vitamin D deficiency was more prevalent in patients with significant CAD (2142, 67.3%) than in patients with non-significant CAD (613, 58.2%). This relationship was statistically significant (p< 0.001) (Figure 1). Mean vitamin D level was lower in patients with significant CAD (27.2±14.8 ng/ml) than in patients with non-significant CAD (29.5±14.8 ng/ml). The difference was statistically significant (p< 0.001) (Figure 2). In patients with significant CAD, patients with higher syntax scores had lower vitamin D (p=0.008, rho: -0.047). Syntax scores were lower in patients with vitamin D sufficiency than in patients with vitamin D deficiency, but the difference was statistically non-significant (p=0.21). There was no significant difference in the number of diseased vessels between the two groups of patients with vitamin D deficiency and patients with sufficient amounts of vitamin D (P=0.106).
We also assessed the relationship between hs-CRP and vitamin D. Mean hs-CRP level in this sample of patients was 1.8 ±2.1 mg/L. We found no correlation between vitamin D and hs-CRP levels (rho=0.04, p=0.204).
We found that vitamin D deficiency was significantly more frequent in men (2499, 70.4%) than in women (1486, 58.6%) (p< 0.001).
Although several studies have reported an association between vitamin D deficiency and CAD, some studies found no such association. In light of the unresolved discrepancies between different studies, we conducted this cross-sectional study of 4234 patients from the general population to search for evidence of this association.
Wang and colleagues, in their analysis of data from the Framingham Offspring Study of 1739 participants who were followed for 5.4 years, showed that vitamin D deficiency was associated with CVD. However, in that study vitamin D deficiency was defined as levels lower than 15 ng/mL, whereas we considered levels lower than 30 ng/mL as vitamin D deficiency [16]. Watson et al. showed that higher serum levels of vitamin D were inversely associated with coronary calcification [17]. In a cross-sectional study of 315 patients by Dhibar et al., the prevalence of vitamin D deficiency was very high but did not correlate with CAD severity [18]. It should be noted, however, that the sample size in their study was small. Chen et al. concluded that low vitamin D levels were associated with CAD severity [19]. These authors assessed the severity of CAD with the SYNTAX score in a sample of 348 patients. Sogomonian et al. showed that serum 25-hydroxy vitamin D concentrations were inversely correlated with the percentage of coronary artery stenosis in their sample of 9399 patients [20]. In another cohort study, Schöttker et al. showed that vitamin D deficiency was strongly associated with an increased risk of cardiovascular mortality [21]. In addition, a metaanalysis by Sokol et al. concluded that there was a modest increase in the risk of cardiovascular events with low levels of 25-hydroxy vitamin D3 [22].
Manousak and colleagues, in their subsequent metaanalysis, concluded that genetically lowered levels of 25-hydroxy vitamin D were not associated with a higher risk of CAD [23]. However, an earlier metaanalysis and systematic review by Elamin and colleagues showed that trial data did not support an association between vitamin D and a reduction in mortality or cardiovascular risk [24]. Pittas et al. concluded that the association between vitamin D level and cardiometabolic outcomes was uncertain [25].
The most notable findings in the present study were that CAD severity correlated with vitamin D deficiency, and that vitamin D deficiency was associated with a higher prevalence of CAD. Another positive aspect of the present study was our comparatively large sample size of more than 4000 patients.
The results of the present study showed that vitamin D deficiency was associated with CAD prevalence independently of hs-CRP level. Ridker et al. concluded that CRP level can be a predictor of cardiovascular events [26]. Haverkate et al. demonstrated an association between high serum CRP levels and the prevalence of coronary events in patients with stable ischemic heart disease and unstable angina [27]. Faivre and colleagues showed that low vitamin D levels were inversely correlated with hs-CRP levels in the general population [28]. However, Milajerdi et al. found that vitamin D level did not influence hs-CRP level [29]. In their metaanalysis, Chen et al. showed that vitamin D supplementation was able to lower hs-CRP levels [30].
In the present study, the mean level of 25-hydroxy vitamin D was significantly higher in women than in men. However, an earlier study of 3879 participants showed that 25-hydroxy vitamin D levels were higher in men. Muscogiuri et al. found that vitamin D deficiency was more common in females than males [31]. Nonetheless, a metaanalysis by Hagenau et al. showed that mean serum levels of vitamin D were higher in women [32]. There were significant association between the level of vitamin D deficiency and age, sex, and DM (table1), which rise the possibility of role of these risk factors as confounding factors in the CAD group. So although the possibility of relation of vitamin D and CAD is very high there may be correlation through these risk factor of CAD, and it warrants further studies to evaluate these associations.
Our findings support a significant association between vitamin D deficiency and the prevalence of CAD independently of hs-CRP level, and a correlation between vitamin D levels and CAD severity. Furthermore, we found that 25-hydroxy vitamin D levels were lower in men, diabetics and older patients. These results thus support the notion that vitamin D deficiency can be a risk factor for CAD.
The sample of patients in our study was from a single region in Iran, and our data were from a single cardiology subspecialty clinic. Because vitamin D levels are influenced by race and region, our findings should not be extrapolated to other samples of patients. Another limitation was that CAD severity was classified only according to the percentage of stenosis, although severity can also be classified on the basis of the type of lesion, number of diseased vessels, and other criteria such as those used in the Gensini score. A further limitation was that this was a cross-sectional study, so we cannot assess the possible causal relationship between CAD and vitamin D. Our recommendation is to perform a randomized controlled study to test the ability of vitamin D supplementation to prevent and treat CAD and its risk factors.
We thank Shiraz University of Medical Sciences for providing ethical review and approval of our protocol, and K. Shashok (AuthorAID in the Eastern Mediterranean) for improving the use of English in the manuscript.
MMP: Gathering data, randomization, writing the article, data analysis
RG: Study conduction, gathering data, randomization, statistical analysis, writing article
RH: Study conduction, randomization, statistical analysis, writing article
MR: Study conduction, gathering data, randomization
AA: Gathering data, randomization
BZ: Gathering data, randomization
MM: Gathering data, randomization
JK: Main researcher, study idea and protocol, study conduction, gathering data, randomization, statistical analysis, writing article

![]()

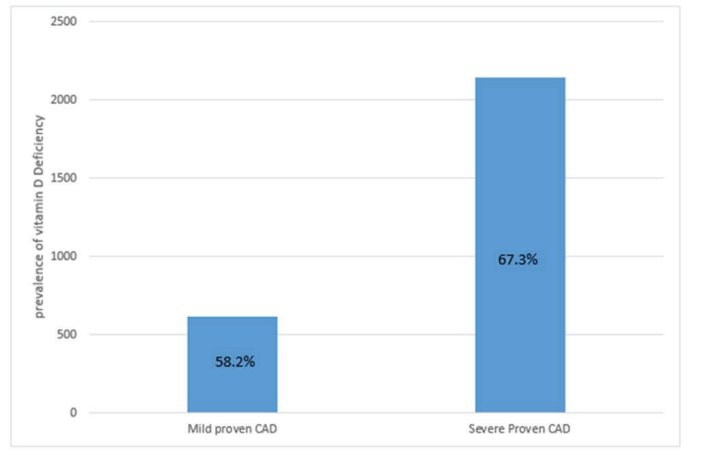 |
| Figure 1: Prevalence of vitamin D deficiency in different CAD groups |
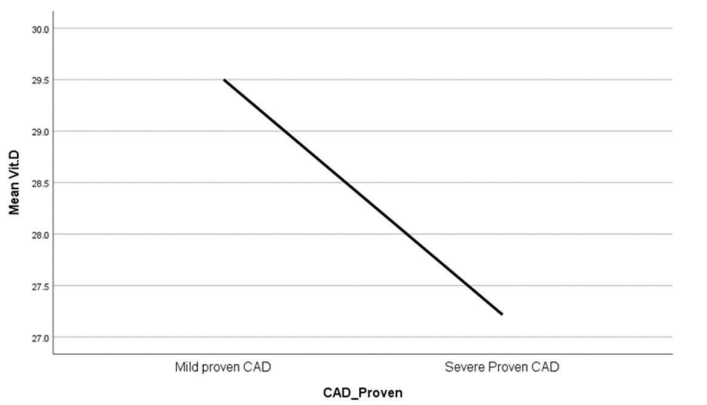 |
| Figure 2: Mean serum vitamin D level in different CAD groups |
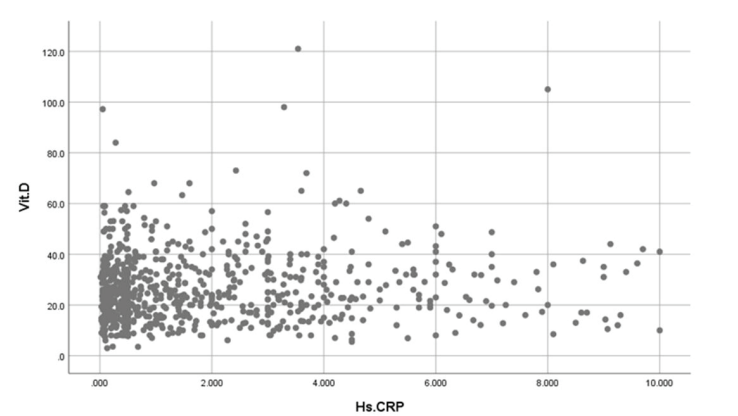 |
| Figure 3: Correlation between serum levels of vitamin D and high-sensitivity C-reactive protein |
|
Vitamin D Deficiency |
Vitamin D sufficiency |
P value |
Age Mean ±SD |
64 ±11 |
67 ±10 |
<0.001 |
Male, n (%) |
1752 (63.6%) |
738 (49.9%) |
<0.001 |
HTN, n (%) |
1429 (51.9%) |
801 (54.2%) |
0.155 |
DM, n (%) |
765 (27.8%) |
466 (31.5%) |
0.011 |
Dyslipidemia, n (%) |
537 (19.4%) |
325 (21.9%) |
0.432 |
|
Vitamin D Deficiency |
Vitamin D sufficiency |
P value |
Syntax, median (IQR) |
19 (12-26) |
17 (12-26) |
0.212 |
Diseased vessels |
|
|
0.106 |
Single vessel disease, n (%) |
858 (40.1%) |
456 (43.9%) |
|
Two vessel disease, n (%) |
527 (24.6%) |
232 (22.3%) |
|
Three vessel disease, n (%) |
757 (35.3%) |
351 (33.8%) |
|




































