Open Access
Research Article
Max Screen
Copyright: © 2021 Drew WL. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
In contrast to previous years which consistently had an influenza “season” our clinical virology laboratory has made only a strikingly small number of identifications of influenza during the early weeks of this respiratory virus season. This experience is similar to its decreased activity in the Southern Hemisphere during their winter, April to July 2020. We report the same experience with RSV. These results are likely attributable to measures employed for control of COVID-19, including social distancing and the use of face masks.
Keywords: Covid-19; Influenza; RSV
Predictions of the impact of influenza A for the winter of 2020-21 have ranged from the possibility of “perfect storm” of COVID-19 and influenza to a virtual absence of influenza. The latter outcome occurred in the Southern Hemisphere during their winter when influenza only rarely occurred while COVID-19 raged [1]. Based on our laboratory experience to date we report that influenza and its partner in crime, respiratory syncytial virus (RSV) are not active and, most likely, will remain at low transmission in the U.S.
Testing for respiratory viruses was performed at the UCSF Clinical Laboratories on specimens submitted for routine testing. Sample types included nasopharyngeal swab, nasal wash / aspirate, tracheal aspirate, bronchial wash and bronchoalveolar lavage specimens. Molecular detection methods included NxTag respiratory pathogen panel (Luminex), Influenza A/B/RSV PCR (Diasorin) and Verigene RP Flex respiratory pathogen panel (Luminex). The RSV assay used the RSV M gene (matrix protein gene) and the influenza assay used the influenza A matrix gene.
Figure 1 portrays the time-course of influenza A and RSV for the years 2010-16 (panels 1-6) as tabulated from PCR results in our laboratory and are the only years in which weekly data was available. The onset of a viral “season” is defined by the first week in which there are two or more identifications in consecutive weeks and are sustained. For RSV the “season” begins at weeks 45, 4 ,45, 46, 46 and 46, respectively in the six years. Influenza identifications begin later in weeks 49, 03, 47, 47, 48, 49 respectively. The end of these “seasons”, while not the subject of this report, is defined by two or more consecutive weeks of <=1 identifications. The average RSV “season” lasts 26 weeks and influenza 19 weeks. Data for weeks 3 to 26 is not provided because our laboratory rarely if ever encounters cases of RSV or Influenza A during those weeks.
In contrast to the above, as of week 2 there has not been a single identification of RSV and very few of influenza A despite 2,735 samples being tested (Figure 2). In each of the prior six years there was at least one specimen for RSV or influenza by week 45. Public health data additionally show minimal detections of influenza at the local, state and national levels [2].
Our results indicate that the SF Bay Area (and likely the rest of the U.S.) will not have its usual seasonal influenza in the winter of 2020-21. While it may seem premature this conclusion is based on our data as presented, however buttressed by this years’ experience in the Southern Hemisphere. During April to July 2020 (weeks 14-31) 0.06% of 83,307 samples tested in Australia, Chile and South Africa were positive where in previous years, 2017-2019 the positivity rate was 13.7% for 175,000 specimens tested in the three countries [1].
The additional important finding in our study is the impact on RSV, a serious pathogen in certain patient populations. It too is unlikely to be active in the winter of 2020-21. Since an average of 177,000 older adults in the US are hospitalized and 14,000 deaths annually are attributed to RSV, its absence would be most welcome [3].
The consistent seasonality which influenza and RSV share for both the beginning and ending of activity is unexplained but suggests the possibility of an interaction or shared factors in transmission cycles. A lesser result of this report is to diminish the need for influenza diagnostics and/or therapy in patients with respiratory illness.
A remaining question is how to explain the absence of these two viruses during the COVID-19 pandemic. Possible explanations include:
This would not account for the inactivity of RSV unless the “viral synergy” theorized previously is operative. Further, influenza vaccine is obtained by less than 50 % of the population and is thus unlikely to have such a profound suppressive effect on the activity of influenza [4]. Influenza vaccination alone has not prevented seasonal peaks in transmission in previous years.
Described many years ago with the observation that infection of an organism with one virus can partially or largely inhibit infection with another virus [5]. The graphs in Figure 1 suggest there is no interference between RSV and influenza at the community level and indeed there may be a synergy as discussed above. Coinfection of individual patients with both viruses have been well described. The possibility of interference of COVID-19 with 2 different viruses seems unlikely but cannot be excluded.
The present study is aimed at appraising the readers of academic history of surgical anesthesia, tale of America's best gift to mankind, journey from hue and cry to calmness and relaxation; and hostility to the wondrous discovery.
The most plausible explanation is that the use of face masks and social distancing, etc. have been more effective for diminishing the spread of RSV and influenza than for COVID-19. Bigerstaff et al, reviewing the literature, estimated that COVID-19 is more transmissible than influenza A [6]. If this explanation is correct, our findings may, in fact, be strong support for these control measures as a general method to prevent respiratory viral transmission. When the inevitable pandemic of a novel influenza variant strikes in the future, these measures may have to suffice until an appropriate vaccine and/or an effective therapeutic is developed

![]()

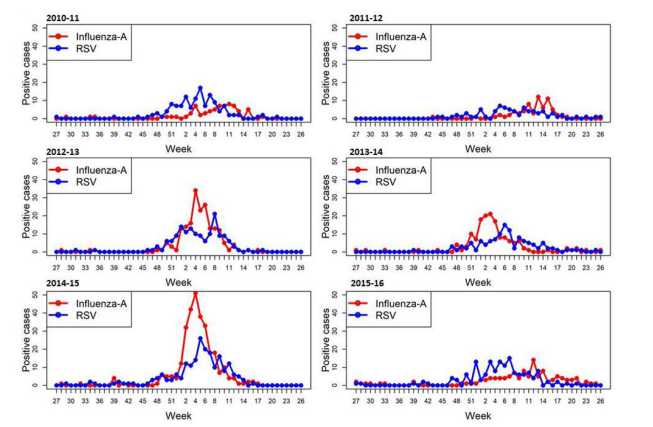 |
| Figure 1: Identifications of Influenza Virus and RSV by PCR in the Clinical Laboratory at UCSF 2010 to 2016 |
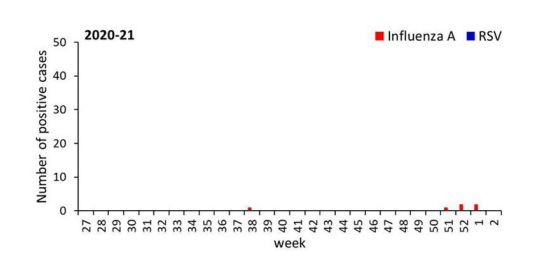 |
| Figure 2: Identifications of Influenza Virus and RSV by PCR in the Clinical Laboratory at UCSF 2020 to 2021 |




































