Open Access
Research Article
Max Screen
Copyright: © 2023 Ayankola Ayantunde. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Substance use is a major health concern in developing countries with associated significant burden and challenges with management. In the management of substance use disorders, significant emphasis is place on motivational interviewing which has been found effective and contributes to well being and positive outcome of care. Therefore how long it takes to make a decision about change and sustain such is very critical in the management of drug use.
Aims:The aims of this study was to determine the pattern of drug use and duration to achieve change talk in drug use management.
Methods:This retrospective study was carried out by extracting information from the individual case records of all in a patient admitted to mental health wards with a diagnosis of mental and behavioral disorder due to psychoactive substance use.
Results:Among the respondents, 78%, 75.6%, 68.3%, 9.8%, 2.4%, 2.4% have problems with the use cannabis, alcohol, tobacco, benzezhol, cocaine. At the period of discharge 63.4% of participants were motivated to change their drug habit. Among the various drugs, those that engage in cannabis, tobacco had 53% and 46.4% respectively of them motivated to change which was statistically significant.
In term of duration of use, those that are motivated had a median value of 10.00 (5.25 – 12.50) years while those not motivated had that of 9.00 (4.00- 12.00) years.
Conclusion:This study have been able to show that nicotine and cannabis are associated with likelihood of becoming motivated to achieve change talk and also duration of use of substance is not a determinant to change talk. First point of contact for substance use disorders treatment appears to be mental health facilities, therefore effective change talk should be reinforce at such places
Keywords: Model of change, Motivational interviewing, Duration to change talk, Drug management
Substance use is a major health concern in developing countries with associated significant burden and challenges with management[1]. The prevalence of substance use is increasing and similarly, the prevalence of those with its disorder is also rising [2]. The number of those that receive orthodox care and present in health facilities is low in Nigeria and even among those that present for treatment, little is known about the nature of treatment and contributing factors to effective treatment [3].
In the management of substance use disorders, significant emphasis is place on motivational interviewing which has been found to be effective and contribute to well being and positive outcome of care [4].
Motivational Interviewing is a client-centered approach to counseling that helps clients overcome their ambivalence or lack of resolve for behavioral change. In a collaborative and supportive setting, counselors elicit motivation to change from the client rather than through direction or persuasion [5]. Previous studies have shown that motivational interviewing is one of the hallmarks of drug use management [6-8]. One of the goals of the management team is to motivate the patient to attained Decision stage in a model of change behavior especially in their attitude to their drug use. This is the stage implementation whereby a client makes a commitment to change. In most hospital setting, the majority of inpatient is in a state of denial to their drug problems and unwilling to seek help or yield to hospital care [5].
Motivational interviewing help patient to move from the following stages in their attitude towards their drug use behavior: A Preparatory stage which includes- pre-contemplating stage, contemplating stage, implementing stage includes- Decision stage, Action Stage, Maintenance stage and relapse(9).
Some of the personal factors associated with drug use problems are Age, gender, marital status, family history of substance use [10-12] however little is known about the influence of these factors in determining how soon a client will attain implementation stage.
Other factors that have been found to affect the care of individuals with substance use are the other comorbid health condition such as depression [13], psychosis [14], sleep problems, hypertension, diabetes, respiratory problems, etc [15]. Generally, co-morbidity is common in drug problem and it negatively impacts the care especially the duration of hospital stay and prognosis. However, it is not yet known whether it also affects how soon decisions are reached to change drug habit.
Reducing the cost of treatment has made it necessary to begin to explore factors that may reduce the period at which decision stage in a model of change is attained [16].
Other likely factors that have been found to be associated with the care of drug use management are the pathway to care which may modify the attitude of the client to the motivation to change [17].
In drug use management the time lag from one stage to the other is important such that the sustainability of an implementation is expected to go a long way in the likely success of the treatment. The risk of relapse has been found to reduce when abstinence is achieved over One year [18]. Therefore how long it takes to make a decision about change and sustain such is very critical in the management of drug use.
MI can reduce the extent of substance abuse compared to no intervention. The evidence is mostly of low quality, so further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate [9].- MI is intended to work through its four main principles(4): (1) ex- press empathy, (2) support self-efficacy, (3) roll with resistance, and (4) develop discrepancy. Empathy involves seeing the world through the client’s eyes. Supporting self-efficacy means that clients are held responsible for choosing and carrying out actions to change. The third principle, rolling with resistance, means that the counselor does not fight client resistance, but “rolls with it.” Statements demonstrating resistance are not challenged. Instead the counselor uses the client’s “momentum” to further explore the client’s views. Lastly, motivation for change occurs when people perceive a discrepancy between where they are and where they want to be. Despite effort to provide treatment for those with drug related problems, little is known about how long it takes for client that have motivational interviewing sessions achieve change talk and importantly what are contributing factor to achieving change talk in a Tertiary Health Facility in developing countries.
Objective:The aims of this study was to determine the pattern of drug use and duration to achieve change talk in drug use management.
This retrospective study was carried out by extracting information from the individual case records of all in a patient admitted to mental health wards with a diagnosis of mental and behavioral disorder due to psychoactive substance use. Information on all the patients over the period was retrieved from their individual case records. This is a major limitation to this study as archive data are flaws with inaccuracies in terms of incomplete data, bias reflecting perspective of the person that obtained the primary data,, exclusion of some data and inaccessibility of raw data. The extracted information was on their demographic details such as age, marital status, religion, employment status.
For all patients, there was initial clerking by a psychiatrist in training and the diagnosis was further reviewed by specialist on call. The management planned was finally decided by the managing consultant. Treatment included pharmacotherapy, individual and family sessions with clinical psychologists, and occupational therapist engage patients in assessment and implement vocational rehabilitation.
Motivational Interviewing: The general objectives of each session were essentially to achieve the goal of motivational interviewing. These include establishing therapeutic alliances, helping clients to be aware of the overall and specific consequences of substance use. Also it was to assist them to understand the discrepancy between patients’ current substance use behavior and their future goals and aspiration, help patients re-evaluate their substance use behavior, increase self-efficacy for changing substance use, and assist with goal-setting and creating a change plan. In addition, Each of the Session were framed to patients’ individual level of readiness to change, reasons for substance use, social and environmental influences, negative consequences of substance use, and interaction of substance use with the patient's specific psychiatric disorder(s). After each section there was a review and feedback of what was discussed and progress made with the client. Another section was schedule with the client on agreement, subsequent session start with updates on previous session. In the course of the each session change talk about taken action about the substance use was explored and this was the time patient was considered to be motivated towards it substance use. Level of readiness to take action by the patient was score on a scale of 1 to 10 with a score above 5 implying client was motivated. Finally, therapists assisted patients in creating a change plan that included specific behavioral goals, names of individuals who would provide social support for change and how to overcome barriers to change for those at higher levels of readiness to change and more preparatory, behavioral goals for those at lower levels of readiness. As the intervention emphasized personal goal choice, therapists did not insist on a goal of abstinence although abstinence was implied as a preferred goal.
About 34% of the respondents were between the ages of 25 -29years. 68% stop their education at college level and 41% were unemployed. The median duration of use of substance was 9.50 years (5.00-12.00) while, their median duration from admission to motivation (change talk) was 37 days (22.75-65.75). Concerning the pathway to care, about three quarter of participant have received some form of treatment in an orthodox setting care prior to care in mental health facility. In term of functionality 40% of participants were able to sustain their functioning after discharge. See Table 1
Among the respondents, 78%, 75.6%, 68.3%, 9.8%, 2.4%, 2.4% have problems with the use cannabis, alcohol, tobacco, benzezhol, cocaine. At the period of discharge 63.4% of participants were motivated to change their drug habit. See Figure 1&2
63.4% of clients were with change talk. Participant age 25-29 and those ages 35-39 had 71.4% of them motivated to change their pattern of drug use. Almost half of those with secondary education were rather in sustaining talk. The highest proportion of those motivated to change with respect to their job were Artisan (77.8%), students (75%), trader/farmer (66.7%), while with civil servants, unemployed had about half motivated.
Among the various drugs, those that engage in cannabis, tobacco had 53% and 46.4% respectively of them motivated to change which was statistically significant. Those that take alcohol, tramadol, Benzezhol had 61.3%, 75%, and 100% respectively motivated to change their drug pattern however these were not significant statistically.
In term of duration of use, those that are motivated had a median value of 10.00 (5.25 – 12.50) years while those not motivated had that of 9.00 (4.00- 12.00) years. See Table 2
This research work has made effort to look at the model of change using motivational interviewing among admitted patient in mental health facility. Results of the mean duration of substance use of 9.50 years and the mean age of the participants (31.71 ± 9.15) in this study shows that most of the participants use substances for long before seeking treatment or help for it use and also it may be inferred that many of the subjects started using substance when they were young which may have accounted for the worsening and severity of the illness. This pattern is similar to extant studies [19, 20,21] with similar findings. Some of these attributes early age of use to impair reasoning associated with developing brain with associated impulsivity, experimentation and peer influences. Many times they are not attended to, with some believing that it is part of youthful exuberance which will be outgrown.
Interestingly most of the participant has been to other health care facility for treatment prior to presenting in mental health facility. This is quite different from pathway to care with other non substance use illness such Schizophrenia [21], epilepsy [22] and other mental illness [23] whereby majority first contact for treatment is unorthodox care. It may be explained that substance use problems are most times attributed to lack moral control and also belief that substance abuse is biological in origin and once patient stops the use of substance, they will be well [24]. On account of this, they are better manage in a health institution while psychosis and mood problems are regarded to as Spiritual attack and consider to be better manage in religious or traditional home [25].
This study has been able to show that 63.4% of those that use substances achieved change talk prior to discharge. Motivational interviewing is an established client oriented assessment and an important psychological treatment that help individuals with drug use substance to decide to change their behavior about their substance use. This further support previous studies [26, 7] that have highlighted the effectiveness of motivational interviewing in helping client to achieve change talk.
Importantly, in terms of the various factors associated with motivation to change talk, age was found to be a determinant of the change. Individuals with age of 25-29 years and 35-39 years were with the highest proportion with motivation. At the age of 25 -29years, there is a rising demand for maturity when year loss to substance use behavior begin to make sense and most times youth desire to get married, get sustain a job and as more or else seek for industry and intimacy as explained by Maslow theory. Also at the age of 35 -39 years change become a desire to leave a good legacy for the future.
In term of duration of use of substance, motivation was not significantly determine by length of substance use and there was rather minimal difference between duration of substance use among those motivated and those not motivated. Therefore from this study, long term of use is not a strong determinant of likelihood motivation. However, this differ from other studies [27, 28] that mention that long duration of use negatively correlate with treatment but the extent of this was describe to be indirectly related with treatment outcome [7]
Delay in drug treatment in mental health facility is quite common among those that present in psychiatric unit [29, 30]. This is similar to that found in this study with a three quarter presenting first in non - psychiatry care facility. This reflects the level of knowledge and attitude of caregiver to the cause, nature of illness, and treatment most suited for substance use disorders. This further reiterate the need to integrate and collaborates with various gate keepers of mental health in the community to ensure client receive proper care and referral as needed. At Post discharge period of 6 month, fair proportion of those that receive treatment were able to sustain their functioning which was better than prior treatment however the functioning varies in degree.
Long duration in treatment has being found to be a predictors of positive outcome in substance use management and in this study it was found that averagely it takes about 37 days for those that got motivated to achieve this. Other studies [31, 32] have highlighted that effective treatment takes time and in some cases the whole process could last months or year. Though entry the change model is the first part of drug treatment however, completion and retention ship in recovery is the goal. This is important because effective motivational interviewing can shorten entry time into change model, admission period, delay relapse and improve outcomes.
Among the various drugs, those that engage in cannabis, tobacco had 53% and 46.4% respectively of them motivated to change which was statistically significant. This is similar to a meta –analytic review among adolescents by Jensen et al. [26] and another study by brown et al. [7] that show motivational interviewing significantly brought about change in latency to return to substance use and frequency of use of cannabis in 6 month period after discharge which was not significant with alcohol. This buttress the point that those that take cannabis or tobacco has higher chances to be motivated to change their drug use habit as compare with other substances. The reason for this may be because of the society frown more with the use of cannabis than other drugs. Also, as the clients regain insight to their illness and could understand the strong link between cannabis and psychosis, which most time is responsible for their admission, they may begin to give consideration to readiness of change. Those that take alcohol, tramadol, Benzezhol had 61.3%, 75%, and 100% respectively motivated to change their drug pattern however these were not significant statistically. This may be because of the society attitude towards these substance and also because they are licit drugs.
As other studies [8,9,26] have posited that motivational interviewing improve well being after discharge, this study finding of almost half functioning well at 6 month post discharge is in consonance with these previous studies.
The findings of this study may help policy makers and clinicians to understand that cannabis use disorder and Nicotine Use Disorders are in identified contributing factor to change talk. Further research work may be done to evaluate the reason behind this. This will also help in judicious use of scarce resources in terms of utilization of motivation interview. The result of latency to change talk may also guide those involve Health Economics and planning to effectively plan recovery of clients.
Change talk is critical to management of drug related problems and understanding determinants to duration to achieve this is critical in developing countries with limited resources is necessary. This study have been able to show that nicotine and cannabis are associated with likelihood of becoming motivated to achieve change talk and also duration of use of substance is not a determinant to change talk. First point of contact for substance use disorders treatment appears to be mental health facilities, therefore effective change talk should be reinforce at such places.

![]()

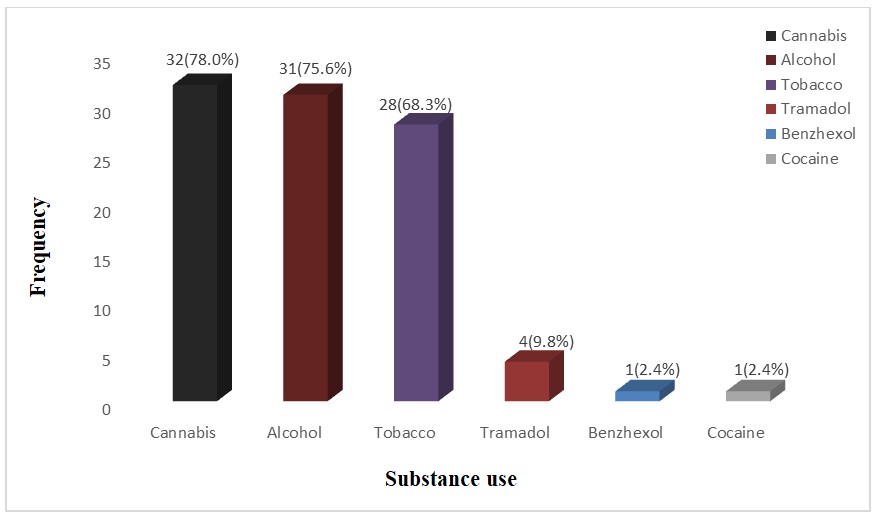 |
| Figure 1: Demographic of psychoactive Substance use |
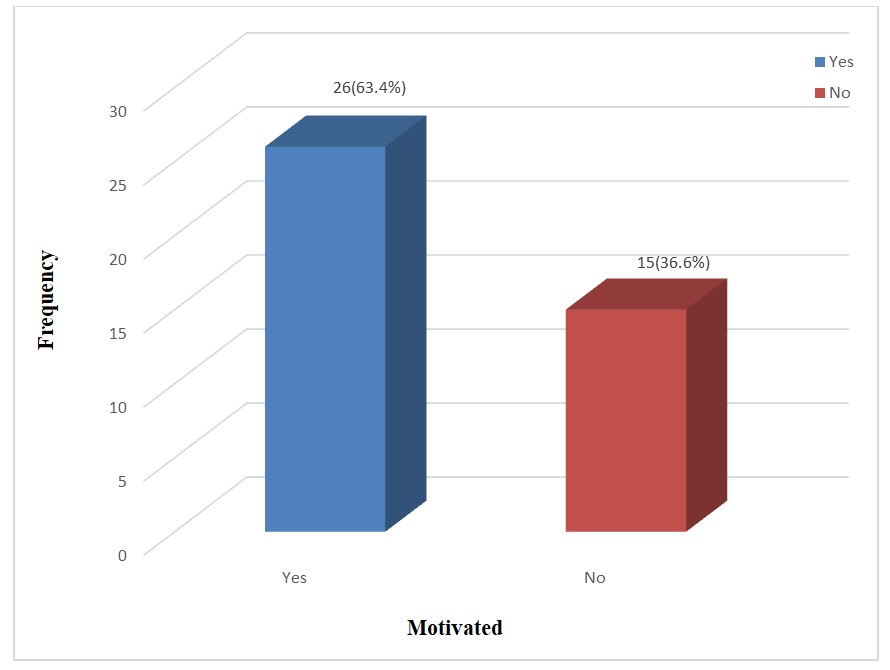 |
| Figure 2: Demographic of Change Talk |
Variable |
Frequency (n = 41) |
Percent |
Age (years) |
|
|
20 - 24 |
7 |
17.1 |
25 - 29 |
14 |
34.1 |
30 - 34 |
6 |
14.6 |
35 - 39 |
7 |
17.1 |
≥ 40 |
7 |
17.1 |
Mean ± SD |
31.71 ± 9.15 |
|
Sex |
|
|
Male |
41 |
100.0 |
Educational status |
|
|
Primary |
3 |
7.3 |
Secondary |
28 |
68.3 |
Tertiary |
10 |
24.4 |
Occupation |
|
|
Artisan |
9 |
22.0 |
Trader/farmer |
3 |
7.3 |
Civil servant |
4 |
9.8 |
Student |
8 |
19.5 |
Unemployed |
17 |
41.5 |
Religion |
|
|
Christianity |
36 |
87.8 |
Islam |
5 |
12.2 |
Duration of substance use (years) |
|
|
Median (IQR) |
9.50 (5.00 – 12.00) |
|
Duration before motivation (days) |
|
|
Median (IQR) |
37.00 (22.75 – 65.75) |
|
Variable |
Frequency (n = 41) |
Percent |
Pathway to care |
|
|
Orthodox |
30 |
72.7 |
Non-orthodox |
11 |
27.3 |
Functionality ( At 6 months) |
|
|
Good |
16 |
40.2 |
Poor |
24 |
59.8 |
|
Motivated |
|
|
|
|
|
Yes |
No |
Total |
χ2 |
p value |
Variable |
n (%) |
n (%) |
n (100.0%) |
|
|
Age (years) |
|
|
|
|
|
20 - 24 |
4 (57.1) |
3 (42.9) |
7 |
0.193 Y |
0.996 |
25 - 29 |
10 (71.4) |
4 (28.6) |
14 |
|
|
30 - 34 |
3 (50.0) |
3 (50.0) |
6 |
|
|
35 - 39 |
5 (71.4) |
2 (28.6) |
7 |
|
|
≥ 40 |
4 (57.1) |
3 (42.9) |
7 |
|
|
Educational status |
|
|
|
|
|
Primary |
3 (100.0) |
0 (0.0) |
3 |
1.875 Y |
0.392 |
Secondary |
15 (53.6) |
13 (46.4) |
|
|
|
Tertiary |
8 (80.0) |
2 (20.0) |
10 |
|
|
Occupation |
|
|
|
|
|
Artisan |
7 (77.8) |
2 (22.2) |
9 |
1.049 Y |
0.902 |
Trader/farmer |
2 (66.7) |
1 (33.30 |
3 |
|
|
Civil servant |
2 (50.0) |
2 (50.0) |
4 |
|
|
Student |
6 (75.0) |
2 (25.0) |
8 |
|
|
Unemployed |
9 (52.9) |
8 (47.1) |
17 |
|
|
Religion |
|
|
|
|
|
Christianity |
23 (63.9)) |
13 (36.1) |
36 |
0.106 Y |
0.745 |
Islam |
3 (60.0) |
2 (40.0) |
5 |
|
|
Substance use |
|
|
|
|
|
Cannabis |
17 (53.1) |
15 (46.9) |
32 |
6.653 |
0.015 F |
Tobacco |
13 (46.4) |
15 (53.6) |
28 |
10.982 |
0.001 F |
Alcohol |
19 (61.3) |
12 (38.7) |
31 |
0.247 |
0.720 F |
Benzhexol |
1 (100.0) |
0 (0.0) |
1 |
0.591 |
1.000 F |
Tramadol |
3 (75.0) |
1 (25.0) |
4 |
0.256 |
1.000 F |
Cocaine |
0 (0.0) |
1 (100.0) |
1 |
1.777 |
0.366 F |
Duration of substance use (years) |
|
|
|
|
|
Median (IQR) |
10.00(5.25-12.50) |
9.00(4.00-12.00) |
|
182.500U |
0.880 |




































