Open Access
Research Article
Max Screen
ISSN: 2456-5504
Copyright: © 2021 Negi PS. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:Non-uniform native T1 (T10) distribution influences reliable measurement of Ktrans: a pharmacokinetic param- eter (Ktrans) that quantitatively measures neovascularization of the tumor tissue that has been used for the classification of malignant breast lesions and to monitor therapy response.
Purpose:To develop a method to assess spatial inhomogeneity of native T10 relaxation time in dedicated mMR breast coil and adopt corrective measure to normalise native T10 values of breast tissue.
Methods: In-house designed multiple tube phantoms, containing gadolinium (Gd) solution were placed in breast coil cuffs which fill the cuff space.
T10 at various spatial locations was calculated by applying dual flip angle (20 and 150) image protocol. The correction factors were derived from the deviation of T10 value from centrally placed phantom in each breast coil to achieve global T10 homo- geneity. The calculated T10 values were normalized by applying correction factors. Correction factor so derived was applied in 46 patients who were undergoing screening MRI and turned out to be normal, to assess its effect on the spatial distribution of T10 value in fat and fibroglandular tissue in the breast.
Results: Post correction, greater homogeneity was achieved with in the breast coil space with uniformity of T10 distribution in phantom at different spatial location (P value: 0.091 corrected vs 0.00049 uncorrected); and the breast tissue with P value for glandular tissue 0.542 and fat 0.414 post correction vs 0.0003* and 0.00001* pre correction respectively.
Conclusion: Significant homogeneity of T10 distribution in normal breast tissues can be achieved by applying correction factors derived with multiple tube phantom-based technique.
Keywords: DCE-MRI; Native T1 (T10); Uniformity; mMR Breast Coil; Multiple Tube Phantom
List of abbreviations: GD: Gadolinium; DCE-MRI: Dynamic Contrast Enhanced-Magnetic Resonance Imaging; PK: Pharmacokinetic; RF: Radiofrequency; FOV: Field of view; DFA: Dual Flip Angle; mMR: Molecular Magnetic Resonance; MRI: Magnetic Resonance Imaging; PET/MRI: Positron emission/ Magnetic Resonance Imaging; Gd- DTPA: Diethylenetriamine pentaacetic acid gadodiamide; ROI: Region of Interest; VIBE: Volume interpolated body examination; ms: Milliseconds; mm: Millimetres; MPR: Multiplanar reformation; VFA:Variable flip angle; IR: Inversion recovery
Breast cancer is the most commonly diagnosed cancer in females [1]. Dynamic Contrast Enhanced-Magnetic Resonance Imaging (DCE-MRI) of Breast provides morphological and angiogenic information which is helpful to differentiate between benign and ma- lignant tissue [2-4]. This technique acquires T1-weighted images prior and post administration of Gadolinium (Gd) contrast agent which provides microvascular properties of the tumor tissue, by calculating time varying signal intensity curvesThese time varying signal intensity curves in routine DCE-MRI derived from high spatial resolution but low temporal resolution images acquired in order of a minute or so Lesions can be differentiated into three types based on time intensity curves; 1) Wash in and wash out (curve type 3) denoting malignant characteristic, 2) Initial rise and Plateau (curve type 2) denoting indeterminate: either benign or malig- nant characteristic, and 3) Persistent rise (curve type 1) denoting benign characteristic [5-11].
High temporal resolution DCE-MRI with few seconds per frame enables quantitative pharmacokinetic (PK) modeling of contrast agent uptake [12]. However, PK parameters is influenced by T10 (msec) and at the same time T10 is influenced by several extrinsic factors including nonlinear RF amplifier due to RF-inhomogeneity, incorrect power setting of 900 pulse, distortions in slice profile, B1 inhomogeneity and flip angle used in MR sequence. B1 inhomogeneity is known to be more critical in higher field strengths e.g. at 3.0T B1 variations across the breasts of patients have been reported around 33%–40% [13, 14]. Kuhl et al. observed in their study that the presence of B1 inhomogeneity was due to the large field-of-view (FOV) and the off-centered positioning of patients. They reported significant differences in B1 values across the FOV between right and left breast. The reduction in intensity of contrast en- hancement in breast tissue had also been reported with reduction in B1 [15].
B1 inhomogeneity is known to effect accurate calculation of PK parameters [16]. B1 inhomogeneity observed across the FOV, affects the actual flip angle (i.e. flip angle error) and finally leads to substantial variations in the value of T10 across the breasts. Studies have reported multiple methods to homogenize the magnetic field by adapting specialized coils, shimming based technologies or by the correction of B1 map [17-20].
Bedair R et al, 2016 [18] used the B1 mapping method for inhomogeneity correction which was subsequently used for calculation of native T10 maps first without B1 correction and then after B1 correction on a 3T system. This study signified the importance of cor- recting B1 so that error should not be translated in subsequent analysis of PK.
We adopted an innovative method to homogenize the physical space with the help of in-house designed multiple tube phantom using DFA (Dual Flip Angle) protocol.
The T10 values were normalized in the mMR breast coil-cuff by applying correction factors derived for each spatial location by using multiple tube phantom placed in each coil cuffs as external standards
The current work has been designed to note the pattern of T10 inhomogeneity, and to see the influence of the spatial correction at multiple locations to achieve global homogeneity in the mMR breast coil for the validation in breast MRI patients.
This study was performed on simultaneous PET/MRI Biograph mMR (Siemens, Erlangen, Germany) by using mMR breast coil (4 channels). We had used prototype in-house designed multiple tube (19 tubes) phantom for each side of breast coil-cuffs. These mul- tiple-tube phantoms were placed to fill the imaging field of dual breast coil cuffs to measure T10 values in various planes, which was used for global T10 normalization across the coil. Our patient group consists of 46 women (mean age 49 years, range 31 to 77 years: 26 premenopausal and 22 post premenopausal) who had undergone screening DCE-MRI between January 2018 to October 2019 and reported to have no breast lesion. The study protocol was approved by the ethics body of the institute and consent of all participating patients was taken.
Phantom tubes were filled with contrast solution i.e. water and Gd-DTPA [(diethylenetriamine pentaacetic acid gadodiamide {Om- niscan}); 0.1 mMol] mixed in the ratio of 10:1 [19]. Each phantom contains 19 tubes, which were arranged in 5 rows containing 3,4,5,4 and 3 tubes in 1, 2, 3, 4 and 5 rows respectively. The dimension of the tube was 16cm x 4cm (length x diameter) and each tube was at a gap of 2cm on a porous thermocol support surface. The arrangement of tubes was done in this manner, so that phantom would be best fitted in the breast coil. These phantoms were placed vertically in each cuff so that tubes would fully occupy cuff space of the breast coil (Figure 1).
Multiple tube phantoms were placed in breast coil cuffs which fill the cuff space, and positioned corresponding to the isocenter of the magnet using light localizer. After localizer images obtained in all three coordinates, 20 flip angle proton density and 150 flip angle non-fat-suppressed T1 weighted images (VIBE-Volume interpolated body examination) were acquired for native T10 calculation for phantom experiment TE (Time to Echo) 1.8 ms, TR (repetition time) 5.2 ms, FOV 360 mm, slices 36, TA (acquisition time) 20.7s, resolution 256 x 256 and voxel size 4.4 mm×1.4 mm×4.0 mm. [21, 22]. T10 at various spatial locations calculated by using DFA protocol was normalized to achieve global T10 homogeneity, by applying correction factors at each spatial location. These correction factors were derived by calculating the deviation of T10 value at a spatial location from centrally placed voxels of the phantom in each breast coil. The derived correction factors was applied to 46 normal breast MRI cases to assess the distribution of T10 values in fat and fibroglandular tissues before and after T10 correction. MRI protocols were performed in a fix table position for phantom study and patient’s study. Matrix size of phantom study was kept same as patient’s study. For technical reason, the phantom scans were acquired in coronal plane and the patients scan were in axial plane covering both breasts completely.
The ROI’s were manually drawn over each tube on both the multiple tube phantoms on the 150 flip angle images (number of pixels: 44/ area: 0.22sq/cm) and these ROI’s were copy pasted on 20 flip angle images across all 36 slices.
For the evaluation of T10 values, the non-fat-suppressed T1 weighted pre-contrast 20 and 150 flip angles VIBE series were separately evaluated in phantom and patients. The Native T10 was calculated with the help of equation 1, 2 manually on the excel sheet [23].
Equation 1 
Equation 2 
Sα1 = intensity value at α1 (20 flip angle), Sα2 = intensity value at α2 (150 flip angle), TR= Repetition time, In= Natural Log
As patient’s data was acquired in axial planes and phantom data in coronal planes; therefore, the patient’s images of 20 and 150 flip angles were reformatted and post processed in coronal planes using MPR (Multiplanar reformation) in Syngovia (Siemens) workstation to match patient’s data with the Phantom Data. ROIs were drawn on the 150 flip angle image on visible fatty and normal fibroglandular tissue on breasts for all patients randomly at different locations. The same ROI was copied and pasted on corresponding 20 flip angle images at the same location for calculation of native T10. Both patient and phantom study were spatially synchronized by using Syngovia software for normalizing the T10 at every spatial location in patients. In 20 and 150 flip angle images, intensity values of the fat and fibroglandular tissue in the breast were manually put in an excel sheet and T10 were measured (Figure 2)
As a first step, the mean T10 value of multiple tube phantoms at the center of each coil cuffs were measured as 6.29± 0.22 ms; which was taken as reference to find a deviation factor for each spatial location. Variations in T10 value was documented for each breast coil from latero-medial, antero-posterior and cranio-caudal directions on each side, before and after applying the necessary correction factor to assess achieved normalization.
Inhomogeneity in T10 distribution was noted for bilateral breast coils in the phantom study. This inhomogeneity was corrected by applying a correction factor for each ROI locations using the following equation
Equation 3

t1n=Measured T10 Value of phantom,pht1=T10 value (6.29± 0.22 ms) of reference phantom,cfn=Correction Factor at each spatial location, n= Multiple tube phantom (1, 2,….19)
The formula used for correcting the T10 value
Equation 4

ct1n= Corrected T10,cfn= Correction Factor,uct1n= uncorrected T10
Two tail T-test was performed between corrected and non-corrected T10 value at every spatial location of the breast coil for both phantom and patient’s study (fat and fibroglandular tissues). The statistical analysis was performed using the MedCalc statistical software package (version 19.8- 64 bit; Windows Vista/7/8/10).
A significant difference in T10 values was observed across ROIs between right & left side of breast coil (p values 0.00049) in phantom study. After correction, a convergence of mean T10 value with regression of standard deviation (SD) was observed suggesting no significant difference (p value 0.091) across spatial locations in the coils. The mean T10 value before correction was 6.08±1.02 ms and 5.38±1.06 ms in right and left breast respectively, which after correction was changed to 6.12±0.26 ms and 6.03±0.28 ms. A detailed distribution of T10 values in breast coil was given in Table 1 and Figure 3.
A significant difference in mean T10 values in fat and fibroglandular tissue was observed between right and left sides of the breast coil before correction. Following correction, no significant difference in T10 relaxation time at different spatial locations was noted. In normal fibroglandular tissue, the mean T10 value before the correction was 1552.79±684.46 ms and 1007.81±420.13 ms in right and left breast respectively, which after the correction was changed to 1418.98±483.67 ms and 1386.17±482.60 ms. For fat tissue, the mean T10 was changed from 398.67±47.37 ms and 326.90±93.40 ms to 388.30±9.41 ms and 390.33±13.91 ms for right and left breast respectively after correction. There was no significant difference in the corrected T10 values of fat tissue (p value 0.41) and fibroglandular tissue (p value0.54) of the right and left breast (Table 2, Figures 4 and 5).
Reliable estimation of native T10 of tissue under investigation is a prerequisite for accurate measurement of pharmacokinetic parameters. This assumes importance because of increasing application of PK parameters to assess the neoangiogenesis property of cancer and in particular its application in breast cancer diagnosis [13,14,17]. One major challenge for mitigating non-uniformity of T10 distribution is inhomogeneity of radiofrequency transmitted field (B1) [18], its influence on VFA (variable flip angle) which causes substantial deviation (≈52%) in the T10 value of fat. Nonuniformity of the B1 at 3T has been reported to affect T10 measurement across the breasts and pose as a challenge for use in quantitative DCE-MRI [24]. Bedair R et al, 2016 [18] also highlighted the influence of B1 at the spatial variation in flip angle across the FOV in a 3T system that is particularly relevant to PK analysis. Development of specially designed volume coils and the use of B1-insensitive adiabatic pulses [25] have demonstrated a substantial effect on the results of quantitative DCE analysis of breast tissue at 3 T [18]. These methods can be specific to a vendor or require specialized software [17-20]. Tsai et al 2017 [17] reported the variations of the average flip angle as 119% and 97% in left breast and right breast respectively, with an overall 22% difference between the two sides on 1.5-T MRI. They used with and without computed B1 corrected VFA to correct T10 value and compared pre-contrast T10 relaxation time in fat and breast tumors.
Pineda et al. (2016) [19] used VFA and multi-inversion recovery (IR) method with reference tissue method and showed accurate B1 map on phantom data. The pharmacokinetic modelling techniques were used to calculate native T10 of the phantom at voxel based spatial positions. Before B1 correction, the average absolute difference between VFA and IR values was 58% ± 21% (p < 0.05); that reduced to 8.1% ± 7.8% (p > 0.05) post correction. In the voxels with maximum difference (10% to the maximum) obtained after correction, the average values estimated to be 170% ± 53% without B1 correction that significantly decreased to 28% ± 13% after correction.
In order to circumvent externous and machine hardware impact, in an innovative approach Jena et al. 2013 [21, 22] attempted to correct T10 by using a single phantom for correction of breast coil. However, this study had an inherent limitation as it uses a single tube phantom for global normalization of T10. In the current study, an ensemble of 19 tubes was used to make the single phantom, which was used to fill the whole cuff space. This enabled us to generate correction factors for each spatial location in the cuff space that makes the technique more robust. The DFA protocol containing 20 and 150 flip angles for native T10 estimation both for phantom experiment and patient’s study, provided better correlative evaluation of the patient data.
We have demonstrated on the phantom study, the effects of T10 normalization on the uniformity of T10 distribution of bilateral breast coil cuffs showing the convergence of mean T10 values across the breast coils with significant improvement in correlation between both sides of coils (p value 0.00049 before correction to 0.091 after correction).
This finding was further verified in 46 clinical cases. The influence of T10 normalization in achieving uniformity of T10 distribution and effect of normalization on mean T10 values in fat and fibroglandular tissue of normal breasts at various spatial locations in bilateral breast coils were studied. Fat is known to be an ideal T10 reference tissue for breast imaging with limited variability [26, 27]. Sung et al. [27] reported the T10 value of fibroglandular tissue on right and left breast to be 1262.8 ± 37.2 ms, 1304.0 ± 104.5 ms respectively at 3.0 T and mean T10 value of 367 ± 18 ms for breast fat with VFA using GRE sequence in 6 patients. Similar results for T10 value for fat and glandular tissues of healthy breasts at 3T have also been reported: 367 ms ± 8 ms and 1445 ± 93 ms respectively in a study of 5 normal breast [28] and 423 ± 12 ms and 1680 ± 180 ms respectively in 6 normal breasts [29], both studies used IR sequence.
The mean native T10 value of the fat tissue and fibroglandular tissue calculated in our study using DFA technique across bilateral breasts following normalization was also found to be in concordance with above reported values [26, 27 and 28]. In addition, we also achieved significant homogeneity in the T10 values for fat and glandular tissue at various spatial locations across different regions of breasts and between both breasts with improved p values.
In summary, significant inhomogeneity in the value of T10 distribution exists between right and left breast coils that can be normalised by using the multiple tube phantom technique adopted in the current study and its portability for application in breast MRI cases. Our findings in normal breast cases are encouraging and with further validation may potentially help improving PK parameters quantification in disease conditions.
We thank Department of Physics, Vivekananda Global University, Jaipur, Rajasthan allowing to carry out this research work as part of the Ph.D. thesis program.

![]()

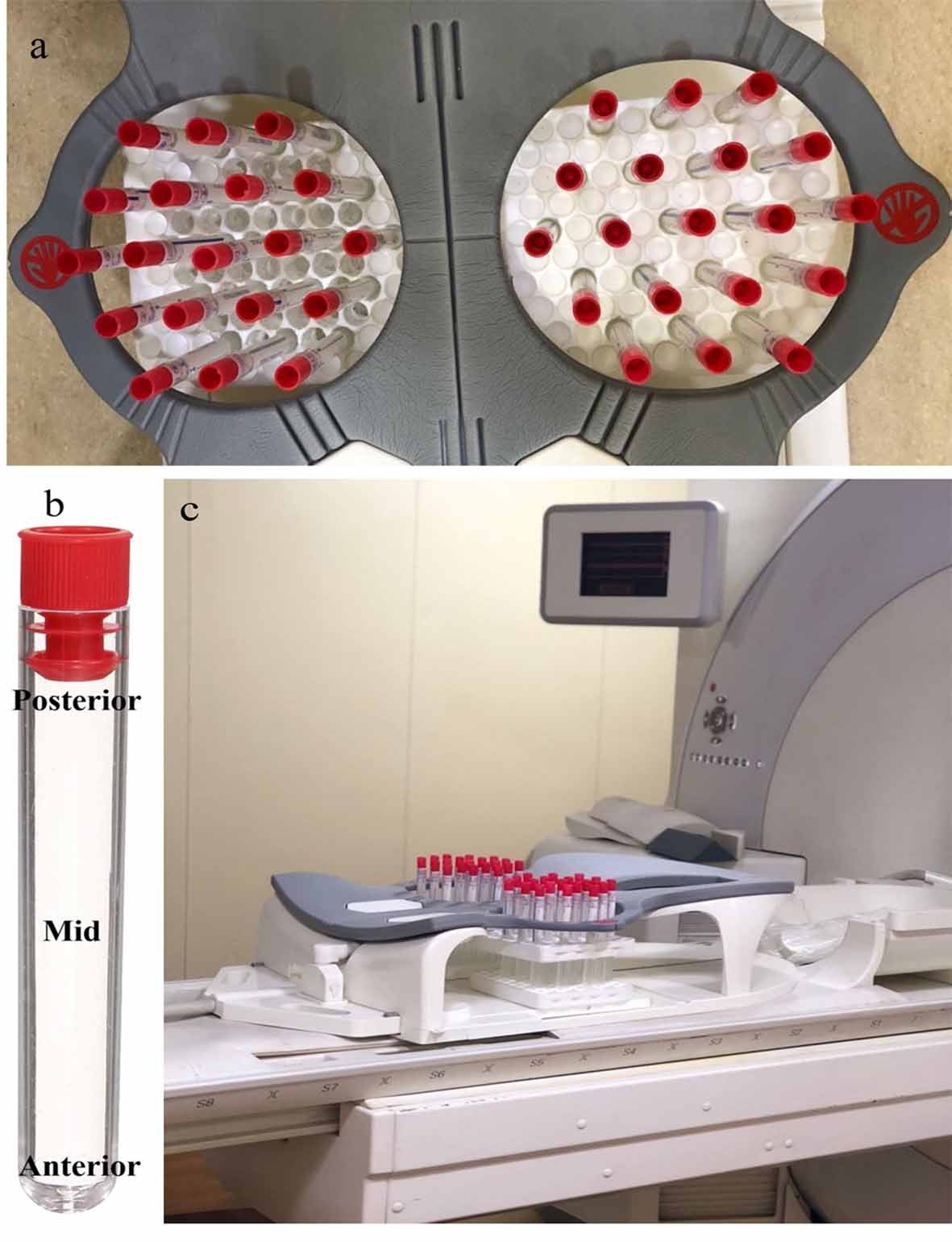 |
| Figure 1: a) In multiple tubes phantom, tubes were filled with GD and arranged as 3,4,5,4 and 3 tubes per row respectively; b) the anterior, middle and posterior part of the phantom tube and c) multiple tube phantom filling the space of breast coil cuffs in Siemens Biograph mMR System |
 |
| Figure 2: Both patient and phantom study was spatially synchronized by using Syngovia software |
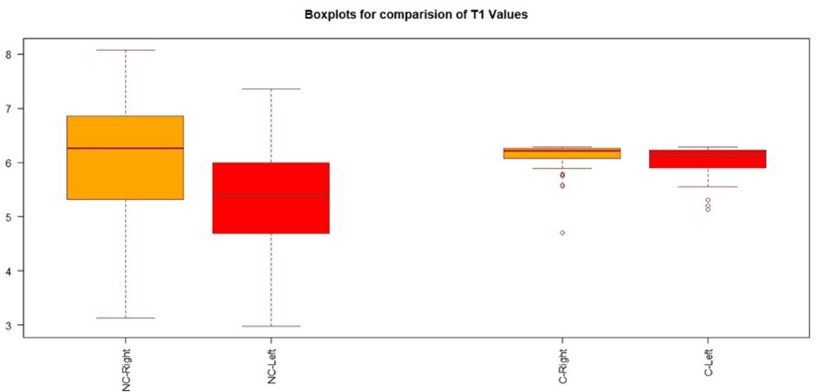 |
| Figure 3: Box plot of uncorrected (NC) and Corrected (C) T10 value distribution of GD phantoms in both breast cuffs |
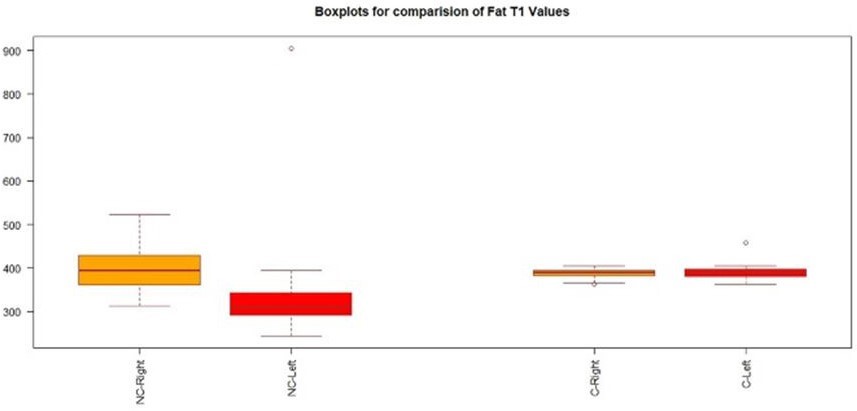 |
| Figure 4: Box plot of mean T10 values uncorrected (NC) and Corrected (C) T10 value in fat tissue comparison in both breasts |
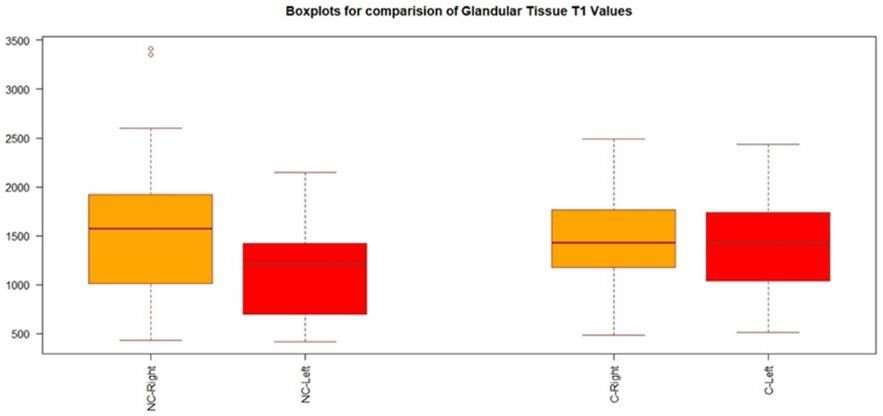 |
| Figure 5: Box plot of mean T10 values uncorrected (NC) and Corrected (C) T10 value in normal fibroglandular tissue comparison in both breasts |
|
Un-Corrected T1 |
Corrected T1 |
||
Tube No. |
Right |
Left |
Right |
Left |
1 |
6.79 |
5.54 |
6.25 |
6.20 |
2 |
6.24 |
6.38 |
6.29 |
6.29 |
3 |
4.80 |
5.80 |
5.94 |
6.25 |
4 |
6.80 |
5.99 |
6.25 |
6.28 |
5 |
6.85 |
7.08 |
6.24 |
6.19 |
6 |
6.71 |
6.82 |
6.26 |
6.24 |
7 |
4.77 |
6.25 |
5.92 |
6.29 |
8 |
7.08 |
5.29 |
6.19 |
6.13 |
9 |
7.61 |
6.90 |
6.01 |
6.23 |
10 |
7.07 |
7.33 |
6.19 |
6.12 |
11 |
5.98 |
7.36 |
6.27 |
6.11 |
12 |
4.19 |
5.42 |
5.59 |
6.17 |
13 |
7.59 |
5.92 |
6.02 |
6.27 |
14 |
7.34 |
6.63 |
6.11 |
6.27 |
15 |
6.79 |
7.09 |
6.25 |
6.19 |
16 |
5.48 |
6.71 |
6.19 |
6.26 |
17 |
6.34 |
5.17 |
6.29 |
6.09 |
18 |
6.33 |
5.74 |
6.29 |
6.24 |
19 |
5.12 |
6.31 |
6.07 |
6.29 |
20 |
6.24 |
4.76 |
6.29 |
5.92 |
21 |
6.18 |
4.72 |
6.29 |
5.90 |
22 |
5.19 |
4.45 |
6.10 |
5.75 |
23 |
6.44 |
5.39 |
6.29 |
6.16 |
24 |
7.01 |
5.60 |
6.21 |
6.21 |
25 |
5.75 |
5.88 |
6.24 |
6.26 |
26 |
4.71 |
5.51 |
5.89 |
6.19 |
27 |
7.34 |
5.18 |
6.12 |
6.09 |
28 |
6.76 |
6.56 |
6.26 |
6.28 |
29 |
7.05 |
6.01 |
6.20 |
6.28 |
30 |
5.73 |
5.68 |
6.24 |
6.23 |
31 |
3.13 |
4.52 |
4.70 |
5.79 |
32 |
6.89 |
5.29 |
6.23 |
6.13 |
33 |
7.01 |
5.50 |
6.21 |
6.19 |
34 |
6.26 |
4.97 |
6.29 |
6.01 |
35 |
4.48 |
5.17 |
5.77 |
6.09 |
36 |
6.27 |
4.62 |
6.29 |
5.85 |
37 |
5.83 |
5.21 |
6.26 |
6.10 |
38 |
4.14 |
5.50 |
5.56 |
6.19 |
39 |
6.69 |
5.02 |
6.26 |
6.03 |
40 |
6.36 |
4.23 |
6.29 |
5.61 |
41 |
6.79 |
4.63 |
6.25 |
5.85 |
42 |
5.98 |
5.96 |
6.27 |
6.27 |
43 |
5.69 |
4.46 |
6.23 |
5.76 |
44 |
5.87 |
4.65 |
6.26 |
5.86 |
45 |
7.09 |
5.55 |
6.19 |
6.20 |
46 |
4.91 |
7.26 |
5.99 |
6.14 |
47 |
6.10 |
5.23 |
6.28 |
6.11 |
48 |
4.45 |
3.59 |
5.75 |
5.13 |
49 |
6.93 |
5.09 |
6.22 |
6.06 |
50 |
8.08 |
4.69 |
5.78 |
5.88 |
51 |
5.22 |
3.80 |
6.11 |
5.31 |
52 |
5.10 |
3.68 |
6.06 |
5.20 |
53 |
4.86 |
4.24 |
5.96 |
5.62 |
54 |
7.16 |
4.79 |
6.17 |
5.93 |
55 |
5.49 |
2.98 |
6.19 |
5.55 |
56 |
5.32 |
3.43 |
6.14 |
5.99 |
57 |
6.30 |
3.02 |
6.29 |
5.59 |
Mean |
6.08 |
5.38 |
6.12 |
6.03 |
SD |
1.02 |
1.06 |
0.26 |
0.28 |
|
UC GT T1(msec) |
C GT T1(msec) |
UC Fat T1(msec) |
C Fat T1(msec) |
||||
|
Right |
Left |
Right |
Left |
Right |
Left |
Right |
Left |
1 |
1703.91 |
1511.26 |
1460.54 |
1446.14 |
394.27 |
363.25 |
373.72 |
380.38 |
2 |
774.69 |
550.73 |
764.73 |
769.34 |
350.64 |
345.57 |
381.90 |
388.60 |
3 |
1985.58 |
1285.73 |
1538.76 |
1538.03 |
386.25 |
332.90 |
390.92 |
398.05 |
4 |
667.67 |
475.22 |
659.09 |
663.86 |
406.49 |
348.56 |
383.06 |
394.31 |
5 |
1620.75 |
1498.11 |
1605.58 |
1620.39 |
352.99 |
332.22 |
398.65 |
405.24 |
6 |
2173.91 |
1608.68 |
2145.95 |
2167.43 |
473.06 |
310.57 |
394.46 |
398.86 |
7 |
681.88 |
1141.61 |
1054.30 |
1092.42 |
333.24 |
327.38 |
392.89 |
387.22 |
8 |
1923.71 |
1104.26 |
1426.35 |
1476.98 |
329.20 |
245.83 |
394.41 |
375.47 |
9 |
1236.72 |
700.60 |
1184.11 |
985.31 |
313.09 |
243.64 |
391.81 |
362.59 |
10 |
1294.17 |
682.91 |
1197.78 |
1043.07 |
388.68 |
297.58 |
393.39 |
381.14 |
11 |
1445.67 |
1430.20 |
1432.14 |
1494.15 |
373.01 |
261.62 |
405.18 |
389.34 |
12 |
1450.88 |
848.37 |
1284.45 |
1252.14 |
343.05 |
308.55 |
381.95 |
380.40 |
13 |
2267.71 |
1366.46 |
1808.16 |
1846.17 |
359.19 |
283.90 |
405.13 |
388.99 |
14 |
3414.93 |
1455.28 |
1549.85 |
1523.91 |
409.67 |
287.41 |
380.17 |
387.24 |
15 |
1445.43 |
1319.47 |
1600.99 |
1626.74 |
361.38 |
311.43 |
393.59 |
390.60 |
16 |
1638.69 |
1418.55 |
1544.81 |
1592.42 |
343.83 |
304.49 |
405.37 |
396.88 |
17 |
429.88 |
518.95 |
556.85 |
589.33 |
385.06 |
304.44 |
393.14 |
386.64 |
18 |
2345.13 |
1377.66 |
1933.87 |
1924.52 |
374.45 |
306.58 |
385.49 |
374.58 |
19 |
1725.40 |
466.54 |
1250.31 |
712.58 |
351.02 |
256.97 |
401.96 |
382.42 |
20 |
864.09 |
449.74 |
769.74 |
686.92 |
418.70 |
313.35 |
382.15 |
391.41 |
21 |
1297.20 |
802.67 |
1189.75 |
1150.07 |
371.47 |
315.11 |
388.40 |
377.72 |
22 |
1381.18 |
685.69 |
1176.27 |
1047.32 |
436.12 |
298.99 |
389.42 |
389.70 |
23 |
959.44 |
1280.86 |
1131.17 |
1178.35 |
341.22 |
343.88 |
390.36 |
390.75 |
24 |
3354.35 |
1406.06 |
2487.11 |
2075.26 |
522.22 |
335.05 |
395.29 |
400.80 |
25 |
2307.16 |
1486.32 |
1831.25 |
1858.03 |
461.53 |
289.57 |
390.10 |
390.15 |
26 |
1343.63 |
1365.45 |
1326.35 |
1359.12 |
428.67 |
373.13 |
381.58 |
399.45 |
27 |
446.96 |
573.95 |
485.59 |
516.47 |
437.87 |
311.94 |
373.65 |
376.57 |
28 |
1613.30 |
1602.57 |
1707.13 |
1746.54 |
396.36 |
351.22 |
381.95 |
399.09 |
29 |
1015.40 |
1221.65 |
1250.59 |
1240.93 |
341.11 |
292.69 |
390.61 |
391.49 |
30 |
1298.82 |
1539.51 |
1623.34 |
1683.77 |
392.74 |
365.68 |
387.40 |
395.59 |
31 |
2457.37 |
2149.68 |
2353.52 |
2431.84 |
398.17 |
394.97 |
394.44 |
405.66 |
32 |
1736.94 |
945.44 |
1663.04 |
1444.05 |
462.31 |
327.99 |
390.75 |
389.87 |
33 |
2597.19 |
1383.24 |
2195.22 |
2041.58 |
370.61 |
293.32 |
365.95 |
373.60 |
34 |
1622.16 |
992.23 |
1413.88 |
1377.28 |
396.86 |
320.16 |
383.63 |
400.12 |
35 |
2111.79 |
1425.81 |
2083.09 |
2065.23 |
413.92 |
302.56 |
383.09 |
397.02 |
36 |
1683.74 |
1507.27 |
1801.90 |
1847.94 |
477.63 |
279.45 |
363.25 |
377.55 |
37 |
1245.96 |
855.62 |
1234.30 |
1187.66 |
403.27 |
288.09 |
380.38 |
378.04 |
38 |
872.38 |
461.16 |
807.40 |
667.97 |
380.08 |
346.45 |
384.68 |
396.17 |
39 |
1895.63 |
905.24 |
1762.49 |
1336.08 |
363.02 |
905.24 |
394.32 |
458.45 |
40 |
1539.70 |
1141.13 |
1342.00 |
1399.05 |
485.26 |
271.42 |
400.16 |
397.86 |
41 |
1958.51 |
1636.82 |
1854.17 |
1851.67 |
419.78 |
307.46 |
374.82 |
394.83 |
42 |
1909.47 |
1218.05 |
1828.24 |
1738.71 |
463.39 |
273.17 |
396.35 |
381.61 |
43 |
544.71 |
561.58 |
642.21 |
732.51 |
420.70 |
345.32 |
396.45 |
398.82 |
44 |
888.46 |
826.60 |
981.89 |
1017.25 |
429.62 |
355.13 |
380.77 |
387.87 |
45 |
1707.04 |
1357.30 |
1685.56 |
1670.37 |
459.38 |
321.56 |
388.28 |
378.32 |
46 |
549.14 |
417.12 |
647.43 |
586.97 |
418.33 |
341.66 |
386.69 |
388.04 |
Mean |
1552.79 |
1107.81 |
1418.98 |
1376.17 |
398.67 |
326.90 |
388.31 |
390.34 |
SD |
684.47 |
420.14 |
483.67 |
482.61 |
47.38 |
93.41 |
9.41 |
13.91 |
P Value |
0.0003* |
|
0.542 |
|
0.00001* |
|
0.414 |
|




































