Open Access
Research Article
Max Screen
ISSN: 2456-5504
Copyright: © 2021 Liuzzi R. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background:Chronic liver diseases (CHDs) are an important public health issue. The presence of significant fibrosis is a hallmark for liver disease staging and prognosis.
Aims:To develop a non-invasive score that can discriminate between patients with or without fibrosis with the aim to avoid liver biopsy
Methods:Forty patients with CHDs who received liver biopsy to stage fibrosis and 12 normal subjects performed also shear wave elastography (SWE) and ELF-test (Enhanced Liver Fibrosis-test). We chose two different outcomes for histological fibrosis (F0-F1 vs F2-F4) and (F0-F2 vs F3-F4). ELF-test and SWE were independent predictors, categorized using ROC analysis. Two scores called SCORE1 and SCORE2 were devised.
Results:The discriminatory values for SCORE1 were SWE>5.62 kPa and ELF-test >9.33 and for SCORE2 were SWE>7.04 kPa and ELF-test 9.33. SCORE1 specificity was 91.7% (CI 77.5-98.2%), significantly greater than obtained using SWE 63.9% (CI 46.2-79.2%; p=0.0013) or ELF-test 83.3% (CI 67.2-93.6%; p=0.1760) separately. SCORE2 specificity was 95.2% (CI 83.8-99.4%). This value was not significantly greater than obtained using SWE or ELF-test 81.0% (CI 65.9-91.4%; p=0.0921) separately.
Conclusion:These preliminary results suggest SWE and ELF-test can be performed for non-invasive staging of liver fibrosis. The results of these two tests grouped in a single score could increase the specificity for the prediction of the histological fibrosis stage. However, to confirm these results other studies are needed.
Keywords: ELF-Test; Shear Wave Elastography; Fatty Liver; Liver Biopsy
Shear Wave Elastography (SWE) uses the measurement of the propagation velocities of acoustically generated shear waves in tis- sue to estimate liver stiffness with the benefit of simultaneous anatomical B-Mode ultrasound imaging. This method is becoming an important clinical measure for the identification of the stage of hepatic fibrosis (Bedossa and Poynard 1996) [7] and its use is also recommended by the clinical guidelines published by the European Federation of Societies for Ultrasound in Medicine and Biology (Ishak, Baptista et al. 1995) [8] and by the World Federation for Ultrasound in Medicine and Biology (Bamber, Cosgrove et al. 2013) [9].
Also, serum biomarkers and, in particular, the combined use of three serum biomarkers of hyaluronic acid (HA), tissue inhibitors of metalloproteinases (TIMP-1) and terminal amino -yl propeptide of type III procollagen (PIIINP) has recently been proposed for the detection of fibrosis. This simplified version of the panel of these biomarkers was called Enhanced Liver Fibrosis (ELF)-test. This non-invasive test has been shown to possess high reproducibility and good diagnostic performance in assessing the degree of hepatic fibrosis (Sarvazyan, Rudenko et al. 1998, Bae, Cho et al. 2010, Yoo, Kim et al. 2013, Miele, De Michele et al. 2017) [10-13]. Our study aimed to evaluate the usefulness of the combined use of ELF-test with SWE to diagnose the presence or absence of hepatic fibrosis and to stage the degree of this pathology.
In our outpatient clinic, we evaluated 40 subjects with chronic liver disease that received liver biopsy and 12 normal subjects (Bravo, Sheth et al. 2001, Angulo, Kleiner et al. 2015, Ekstedt, Hagstrom et al. 2015) [2-4]. The exclusion criteria were other active infectious diseases or pregnancy. Five patients (12.8%) received a diagnosis of liver cirrhosis, 11 patients (28.1%) were diagnosed with viral chronic hepatitis, 7 (17.9%) had alcoholic liver disease and 17 patients (41.2%) exhibited unexplained abnormalities on their liver test results. None of the normal subjects had a history of liver disease and had normal test results; all of them had normal abdominal ultrasonography. All of the subjects received a general abdomen US and Shear Wave Elastography (SWE) examination. The study was approved by the local Ethical Committee of the faculty of Medicine of the University of Naples Federico II. The patients provided written informed consent before the beginning of the study.
A liver specimen was collected with the BIOMOL-16 G, a soft tissue biopsy semiautomatic needle (HS SpA. Aprilia-Italy), using the modified Menghini needle technique. The liver biopsy specimens were fixed in formalin and embedded in paraffin. A special- ized pathologist with more than 20 years of experience who was kept in the dark about the SWE values and clinical information reviewed the biopsy specimens. Only biopsy specimens 2 cm long and with a minimum of 11 intact portal tracts were eligible for evaluation (Cholongitas, Senzolo et al. 2006) [6]. Liver fibrosis was evaluated semi-quantitatively according to the Metavir scoring system (Bedossa and Poynard 1996) [7]. Liver fibrosis was staged using a five-point ordinal scale ranging from 0 to 4 as follows: F0 - no fibrosis; F1 - portal fibrosis without septa; F2 - portal fibrosis with few septa but intact architecture; F3 - numerous septa with architecture distortion without cirrhosis; F4 - cirrhosis. (Ishak, Baptista et al. 1995) [8]. Moreover, ALT levels were used as an index of hepatic inflammation.
Clinical and demographic characteristics of patients and normal subjects are summarized in Table 1.
The Shear Wave Elastography was performed using the iU22 ultrasound system (Philips Healthcare. Bothell. WA. United States) with a convex broadband probe and the ElastPQ® technique. The SWE technique generates shear waves inside the liver using ra- diation force from a focused ultrasound beam. The patient was lying in a lateral decubitus position with the right arm extended above the head to access the right hypochondrium and to increase the intercostal acoustic window (Bamber, Cosgrove et al. 2013, Ferraioli, Filice et al. 2015, Dietrich, Bamber et al. 2017) [9,14,15]. The probe was placed parallel to the intercostal space with sufficient gel to minimize rib shadowing. A ROI (Region of Interest) with a box size of 2.0x1.0 cm2 was positioned within the liver parenchyma under visual control in a two-dimensional B-mode at a depth of at least 2 cm below the liver capsule in segments 7 or 8 of the liver, taking care not to include large vasculature or biliary structures. The sub-capsular regions that usually contain larger fibrotic content were avoided. During scanning between ribs, no pressure was applied to the liver and the patient was asked to stop breathing for a few seconds to minimize motion artifacts. Liver stiffness measurements were performed on the same area of the liver parenchyma. The equipment provides the shear wave velocity (m/s) in the ROI as well as the depth at which the measurement was performed. To compute tissue stiffness in kiloPascal (kPa) the shear wave velocity (v) was converted into the Shear Modulus (G) using the formula
G =ρv2
where: ρ is the density of the tissue (kg/m3).
Fifteen measurements were collected at the same location and a report was generated when a success rate of at least 80% was ob- tained (Fraquelli, Rigamonti et al. 2007) (Roulot, Czernichow et al. 2008) [16,17]. The median of these measurements was used to estimate the degree of liver stiffness for each subject and were correlated with the biopsy Metavir score.
Herrmann et al in a meta-analysis study evaluated the diagnostic performance of SWE in patients with mixed aetiologies (Her- rmann, de Ledinghen et al. 2018) [18]. Their cutoff were: 8.25 for stage 0 and 1 vs 2; 9.15 stage 2 vs 3, and 9.89 for stage 3 vs 4.
The operator was kept in the dark about the results of previous measurements and the biological and histological data.
The ELF-test combines three serum biomarkers: Hyaluronic acid (HA), Procollagen III amino terminal peptide (PIIINP) and Tissue inhibitor of metalloproteinase (TIMP-1). These biomarkers can identify a quantifiable level of liver fibrosis. To calculate the ELF value, the ADVIA Centaur CP immunochemical analyser (Siemens Healthcare Diagnostics, Germany) was used according to the manufacturer’s instructions and the following formula was applied:
ELF=2.494+0.846 In (CHA) + 0.735 In (CPIIINP) + 0.391 In (CTIMP-1).
Where (C) is the concentrations of the biomarkers and each assay is measured in ng/mL (Yoo, Kim et al. 2013, Zarski, Sturm et al. 2013, Miele, De Michele et al. 2017) [12,13,19]. The test result was divided into three bands for the classification of the degree of fibrosis: < 7.7 no /mild fibrosis, 7.7-9.8 moderate fibrosis and >9.8 severe fibrosis (Nobili, Parkes et al. 2009) [20]. All methods were carried out in accordance with relevant guidelines and regulations.
Continuous variables were expressed as the median and range. Categorical variables were expressed as percentages. A receiver operating characteristic (ROC) curve was calculated (Hanley and McNeil 1982) [21]. The area under the curve (AUC) was used to evaluate test accuracy and the discrimination value was determined by Youden’s J statistic (Fluss, Faraggi et al. 2005) [22]. Sensi- tivity and specificity values were computed using the discrimination values as a threshold. All of the statistical tests were two-sided and a p-value of 0.05 or less was considered statistically significant. The statistical analysis was performed using MedCalc software version 12.7 (MedCalc Software Bvba. NL).
We had analyzed data from 52 subjects (40 with CLD and 12 without a history of liver disease). Valid SWE measurements were obtained from all but one CLD subject (measurement failed because of ascites). The demographic, clinical, and biochemical char- acteristics of all the subjects are summarized in Table 1. Age, sex and Body mass index (BMI) were not significantly associated with SWE measurements and Elf-test values. We have chosen to analyze two different outcomes for histological fibrosis: (F0-F1 vs F2-F4) and (F0-F2 vs F3-F4). ELF-test and SWE were chosen as independent predictors. These two variables were categorized using the results of ROC analysis and in particular using the cutoff values. We devised two scores based on these predictors by assigning the value “1” when the value of both predictors exceeded the cut-off value and “0” in all other cases. We called these two novel scores SCORE1 for (F0-F1 vs F2-F4) and SCORE2 for (F0-F2 vs F3-F4).
The ROC Curves obtained from ROC Curve analysis using (F0-F1 vs F2-F4) as the outcome are shown in Figure 1. The discrim- inatory values are SWE>5.62 kPa and ELFtest >9.33 (Table 2). The specificity of SWE is 63.9% (CI 46.2-79.2%; p=0.0013) or for ELF-test is 83.3% (CI 67.2-93.6%; p= 0.1760) (Table 2). The resulting SCORE1, shown in Figure 1, has a specificity of 91.7 % (CI 77.5-98.2%) significantly greater than obtained using SWE and ELF-test separately (Table 2).
The ROC Curves using (F0-F2 vs F3-F4) as the outcome are shown in Figure 2. The discriminatory values are SWE>7.04 kPa and ELFtest >9.33. The SCORE2 is shown in Figure 2.
SCORE2 specificity is 95.2% (CI 83.8-99.4%) (Table 3). This value is not-significantly greater than obtained using SWE or ELF-test 81.0% (CI 65.9-91.4%; p = 0.0921) separately (Table 3).
Assessment of liver fibrosis is important in determining prognosis and disease progression in patients with chronic liver diseases and need to choose the better treatment to apply. Although liver for determining the degree of liver fibrosis the biopsy is the gold standard, issues regarding invasiveness of this technique and a small amount of liver tissue evaluated can limit its applicability and interpretation in clinical practice. To overcome these limitations, non-invasive methods to address liver fibrosis are being increas- ingly evaluated. At the present day, several serum markers are used, as surrogate measurements, for the assessment of liver fibrosis. However, these methods are not free of limitations and many components of the serum panel do not directly reflect or underline this process. Liver fibrosis markers are typically divided into indirect and direct markers of fibrogenesis and fibrinolysis. Indirect markers of hepatic fibrosis include biochemical tests that reflect alterations in hepatic function such as bilirubin, AST, ALT, GGT and platelet count. Direct markers of fibrosis, on the other hand, can be divided into markers associated with matrix deposition, degradation, cytokines and chemokines associated with the molecular pathogenesis of fibrogenesis and fibrinolysis (Joseph 2020) [23]. Among these, Enhanced Liver Fibrosis test proved to be among the most reliable.
ELF test components have also some deficiencies in displaying hepatic fibrosis. Firstly, hyaluronic acid is not specific to the liver. Second, PIIINP can be found in four different structures in serum, PIIINP is not specific to hepatic tissue and reflects global ECM metabolism, like HA. Finally, It has been shown that levels of TIMP-1 increase in hepatic tissue and serum in PSC (primary scleros- ing cholangitis), PBC (Primary biliary cholangitis), biliary atresia, AIH (Autoimmune Hepatitis) patients with fibrosis. Moreover, TIMP-1 has been shown to be not a specific marker for liver tissue and serum levels of TIMP-1 may increase in ALD, hemochroma- tosis (HC), asthma, colitis and coronary heart disease. Each of three parameters are not capable of assessing and evaluating hepatic fibrosis by themselves (Gungoren, Efe et al. 2018) [24].
Moreover, transient elastography is considered one of the most used alternatives for biopsy and is suggested in the management algorithms of main European scientific association guidelines. However, fibroscan has some limitation with a failure rate reached about 14,3 % (Shiina, Nightingale et al. 2015) [25]. SWE has a lower failure rate (Zeng, Zheng et al. 2017) [26] that can be explained by the simultaneous B-mode visualization available during the SWE technique which provides the opportunity to select the proper site for measurement. Moreover, SWE allows selecting a more wide area of analysis with respect to fibroscan. In particular, it is able to obtain useful images for diagnostic purposes also in obese subjects or in the presence of ascites (Osman, El Shimy et al. 2020) [27].
Saravazyan et al (Sarvazyan, Rudenko et al. 1998) [10] first described SWE as an approach to generating shear wave acoustic ra- diation force and measuring the resultant shear wave propagation and shear wave speed to reconstruct an elastic modulus. Point SWE utilizes all the propagation data in 2-D ROI to estimate the shear wave speed in that region (Doherty, Trahey et al. 2013, Barr,Ferraioli et al. 2016) [28,29]. Typically, a singleton shear wave speed matric is reported per measurement and clinical studies have supported using a media value across repeated measurements to report a representative measurement for diagnostic purposes (Ferraioli, Filice et al. 2015, Barr, Ferraioli et al. 2016) [14,29].
In our previous work, we found that the accuracy of a test based on the SWE was 0.77, in diagnosing liver fibrosis in patient with Metavir stages from F2 to F4, while the accuracy was 0.89 for patient with Metavir stage from F3 to F4 (Mancini, Salomone Megna et al. 2017) [30].
This work aims to verify if the addition of the information provided by the ELF-test can improve the results obtained using SWE alone. To do this, we have built two scores based on the combination of SWE results with ELF-test results: SCORE1 and SCORE2 realized using Metavir stages from F2 to F4 and Metavir stage from F3 to F4, respectively.
The diagnostic accuracy obtained with SCORE1 was 0.79, not significantly higher than that obtained using the only SWE, but in return, a significant enhancement of specificity was observed 92% vs 64% (p< 0.004). Similar results were obtained with SCORE2: the difference in the diagnostic accuracy was non-significant (0.87 vs 0.89) while, an enhancement of specificity although non significant (95% vs 81%, p=0.092) was observed. Our results are interesting because a highly specific test is to be used in screening situations. The increased specificity reducing false positive results (Maxim, Niebo et al. 2014) [31] reduces the number of subjects to be proposed for invasive diagnostic techniques or unnecessary therapies. Furthermore, a high specificity is also necessary to verify the presence of a disease that has little clinical evidence.
Our study partially confirms results from previously published studies. Katharina Staufer et al (Staufer, Halilbasic et al. 2019) [32] had shown that for diagnosis of F2, F3, and F3, receiver operating characteristic analysis revealed superior diagnostic accuracy of ELF score (AUC) 0.85, 0.90, 0.90), FibroMeterV2G (AUROC 0.86, 0.88, 0.89), FibroMeterV3G (AUROC 0.84, 0.88, 0.88), and LSM per protocol (AUROC 0.87, 0.95, 0.91) versus FIB-4 (AUROC 0.80, 0.82, 0.81) or NFS (AUROC 0.78, 0.80, 0.79). Proprietary fibrosis panels and VCTE show superior diagnostic accuracy for noninvasive diagnosis of fibrosis stage in NAFLD as compared to FIB-4 and NFS. Ragazzo et al. (Ragazzo, Paranagua-Vezozzo et al. 2017) [33] showed good results for ELF with an AUROC of 0.707 and for ARFI a AUROCs of 0.67 for >F2, 0.74 for > F3, and 0.97 for F4.
Trembling PM et al. (Trembling, Lampertico et al. 2014) [34] evaluated the performance of ELF and Transient Elastography (TE) in detecting liver fibrosis regarding liver histology in a cohort of patients with CHB (n = 182), and compared the performance of these modalities. They demonstrated that, in patients with CHB, ELF has good performance in the detection of liver fibrosis.
Moreover, TE performs better in the detection of severe fibrosis.
The weak point of our work is the sample size. This limitation leads to high confidence intervals and the difficulty of distinguishing between two similar values of specificity or sensitivity. The low number of participants cannot allow to draw definitive conclusions and it is not enough to define cut-off points, therefore, to propose a score usable in clinical practice further studies are needed. These studies will allow highlighting further significant differences in order to distinguish the different levels of fibrosis. SWE and ELF-test can be performed with comparable diagnostic accuracy for non-invasive staging of liver fibrosis. Our preliminary results suggest the use of ELF-test and SWE in a combined score on a screening test could increase the specificity for the prediction of histological fibrosis. Confirmation of this result from studies conducted on larger groups could be a useful tool for the non-invasive clinical approach to detect liver fibrosis. SWE has demonstrated an excellent intra-observer and inter-observer agreement, howev- er, other tissue abnormalities such as edema and inflammation, cholestasis and congestion may interfere with SWE regardless of the degree of liver fibrosis (Fraquelli, Rigamonti et al. 2007, Bae, Cho et al. 2010) [11,16].
The combination of SWE with the ELF test, which provides an assessment of fibrosis in liver tissue by analyzing serum markers related to extracellular matrix metabolism (Rosenberg, Voelker et al. 2004, Fraquelli, Rigamonti et al. 2007) [16,35], could theoretically increase the accuracy of SWE in predicting the level of liver fibrosis.
Ethics approval and consent to participate:The study was approved by the local Ethical Committee of the faculty of Medicine of the University of Naples Federico II. The patients provided written informed consent before the beginning of the study.
Consent for publication:“Not applicable”
Availability of data and materials:“Not applicable”
“The authors declare that they have no competing interests”
The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
This work was supported by the Italian Minister of Health Project Code: RF-2010-2314264.

![]()

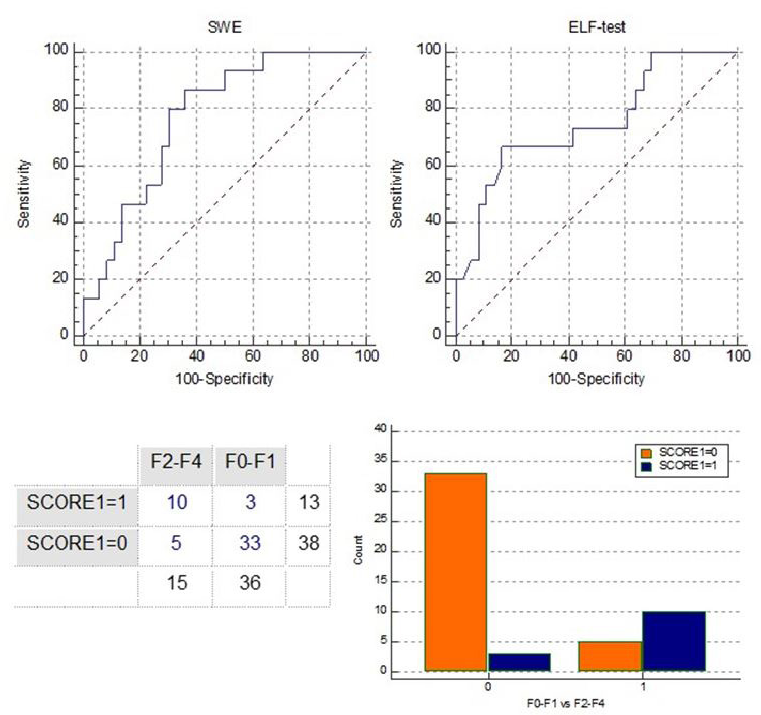 |
| Figure 1: Upper panel) Reciving Operating Characteristic (ROC) curve analysis using (F0-F1 vs F2-F4) as outcome. Lower panel) Diagnostic crosstab for SCORE1 and its representation in bar diagram |
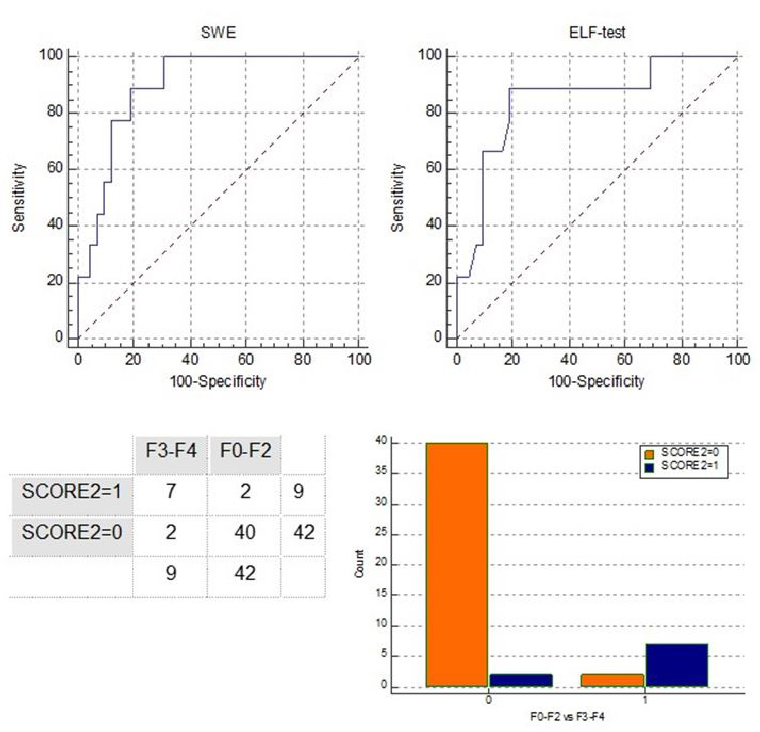 |
| Figure 2: Upper panel) Reciving Operating Characteristic (ROC) curve analysis using (F0-F2 vs F3-F4) as outcome. Lower panel) Diagnostic crosstab for SCORE2 and its representation in bar diagram |
Characteristic |
Subjects (51) |
|
Number (%) |
Male gender |
25 (56%) |
|
Median (range) |
Age (years) |
47.0 (20.0–78.0) |
Weight (kg) |
68.0 (51.0–130.0) |
Body Mass Index (kg/m2) |
24.3 (17.9–38.4) |
Abdominal circumference (cm) |
95.0 (77.0–120.0) |
AST (U/l) |
36.2 (14.0–377.0) |
ALT (U/l) |
45.2 (9.0–577.0) |
GGT(U/L) |
77.6 (14.0–856.0) |
Cholesterol (mg/dl) |
180.0 (62.0–342.0) |
Triglycerides (mg/dl) |
105.3 (27.0–353.0) |
Shear Wave Elastography |
6.15 (2.92–16.66) |
ELF-TEST |
8.93 2.92-13.39) |
Aetiology of liver disease |
Subjects with CHD (39) |
HCV |
4 (10,2%) |
HBV |
7 (17,9%) |
Alcohol-related |
7 (17,9%) |
NASH |
2 (5,1%) |
Others |
19 (48,7%) |
Parameter |
F0-F1 vs F2-F4 |
||
SWE (kPa) |
ELFtest |
SCORE1 |
|
Cut-off |
5.62 |
9.33 |
|
Area under the curve |
0.77 (0.63 to 0.88) |
0.75 (0.61 to 0.86) |
0.79 (0.66-0.89) |
Sensitivity (%) |
86.67 (59.50-98.30) |
66.67 (38.38-88.18) |
66.67 (38.38-88.18) |
Specificity (%) |
63.89 (46.20-79.20) |
83.33 (67.19 -93.63) |
91.67 (77.53-98.25) |
Positive Predictive Value (%) |
50.00 (29.93-70.07) |
65.5 (35.43-84.80) |
76.92 (46.19-94.96) |
Negative Predictive Value (%) |
92.00 (73.97-99.02) |
85.71 (69.74-95.19) |
86.84 (71.91-95.19) |
Parameter |
F0-F1-F2 vs F3-F4 |
||
SWE (kPa) |
ELFtest |
SCORE2 |
|
Cut-off |
7.04 |
9.33 |
|
Area under the curve |
0.89 (0.78 to 0.96) |
0.84 (0.71 to 0.93) |
0.87(0.74-0.94) |
Sensitivity (%) |
88.89 (51.80-99.70) |
88.89 (51.75 -99.72) |
77.78 (39.99-97.19) |
Specificity (%) |
80.95 (65.90-91.40) |
80.95 (65.88 - 91.40) |
95.24 (83.84-99.42) |
Positive Predictive Value (%) |
50.00 (24.65- 75.35) |
50.00 (24.65- 75.35) |
77.78 (39.99-97.19) |
Negative Predictive Value (%) |
97.14 (85.08 to 99.9) |
97.14 (85.08 to 99.9) |
95.24 (83.84-99.42) |




































