Open Access
Research Article
Max Screen
ISSN: 2456-5504
Copyright: © 2021 Jain RD. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Haemangiomas are the most common benign incidentally detected hepatic lesions with a prevalence of ~20%. Most of them have typical imaging features and are easily diagnosed on triple phase studies. These are capillary, flash and giant hemangioma. Another subset of haemangiomas are Sclerosing hemangiomas or atypical haemangioma; these are sclerosed, thrombosed and/or hyalinised due to which these are heterogenous and show varied appearance making them difficult to diagnose.
Most of the times haemangiomas do not need any interventions unless symptomatic, hence it is important for radiologists to be aware of the imaging features and always consider as differential when similar cases are encountered. Here we present two cases of sclerosing hemangiomas in elderly patients.
Keywords: MRI; CT; Hepatic Sclerosing hemangioma
A 71 year old male patient with no comorbidities, complaints of right hypochondriac pain, no weight loss. He was referred to the imaging department for further evaluation. Ultrasound performed showed a heterogenous mass in the posterior segment of the right lobe of liver and was referred to the MRI department for further imaging.
A dynamic post contrast was performed on a 3T MRI Philips Ingenia using Hepatobiliary Specific contrast :Gadobenate disodium Gd-BOPTA.
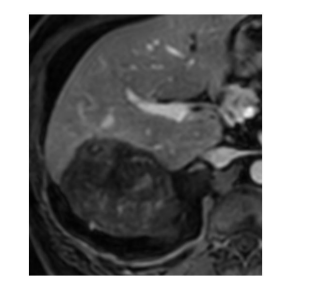
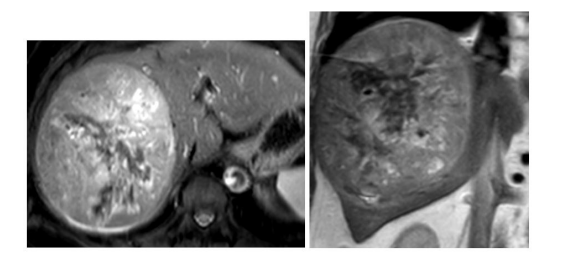
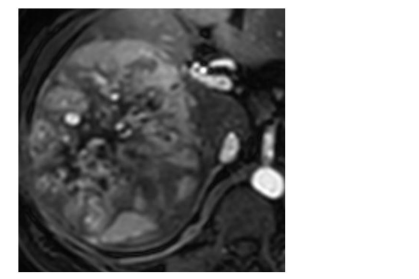
MRI showed significant fatty infiltration of the liver with moderate sized heterogeneous subcapsular lesion in segment VII/VI abutting the right dome of diaphragm. Heterogeneously hyperintense on the T2WI and hypointense on the T1WI. There was associated mild intrahepatic biliary radicle dilatation (Figure 1A, B and C).
The lesion showed varied areas of diffusion restriction and ADC drop (Figure 2A and B) with ADC value in the range of 0.8-1.1x10-3mm2/s.
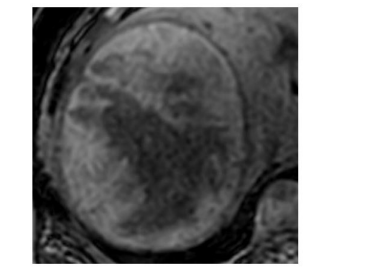
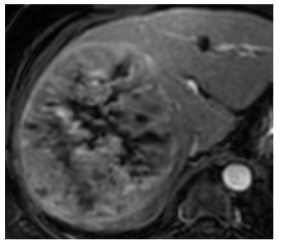
On the dynamic post contrast images the mass showed no enhancement on the arterial phase images (Figure 3). However on the portal phase (Figure 4) and venous phase (Figure 5) there were increased nodular and focal areas of enhancement. Delayed 10mins scan shows heterogenous enhancement of the mass (Figure 6A, B, C, D and E).
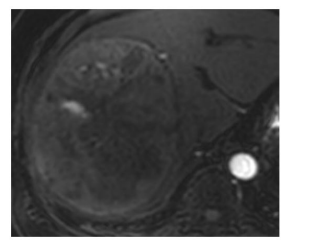
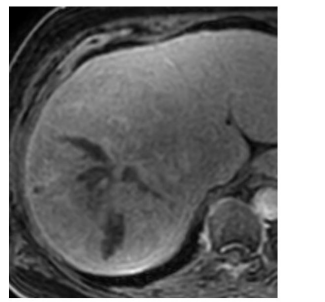
On the 90 min hepatobiliary phase (Figure 7A and B) the mass shows mixed areas of hypointensity and hyperintensity. There was associated capsular retraction and adjacent THID (Transient Hepatic Intensity defect). No regional adenopathy. Another smaller focal lesion was seen in the segment VI. Few simple hepatic cysts were seen. In view of the atypical imaging pattern and a satellite lesion, neoplastic possibility of mixed hepatocellular and cholangiocarcinoma was raised.
In view of the symptoms, age of the patient, heterogeneous pattern and another focal lesion in segment VI with similar enhancement characteristics a decision for resection was made in a multidisciplinary discussion. The patient underwent an uneventful posterior segment surgical resection.
Histopathology (Figure 10A, B and C) confirmed the tumor composed of cavernous thin walled vascular interconnecting channels.The supporting stroma showed hyalinized sclerosis with fibroblasts. Vascular channels were filled with blood. The tumor was unencapsulated, well demarcated from the surrounding liver parenchyma. Histopathological diagnosis of sclerosing cavernous hemangioma was made.
Another case presented is a 65 year old gentleman who came for further evaluation of a focal hepatic mass detected incidentally on the Ultrasound performed elsewhere.The serum AFP and CA 19-9 levels were within normal limits. He was referred for further evaluation to our Imaging department.
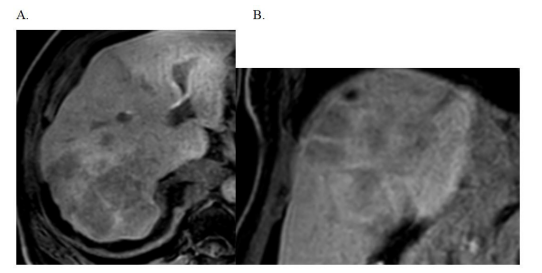
A 3T MRI with hepatobiliary specific contrast (Gd-BOPTA) scan was performed and it showed a heterogeneous mass in the right lobe of liver measuring ~15cms in diameter on T2WI (Figure 11A and B), well defined and well encapsulated. It showed heterogeneous focal vascular enhancement on the arterial phase (Figures 12 and 13);similar to aorta and areas of further enhancement on the portal-venous phase (Figure 14) and the delayed images (Figure 15).On the hepatobiliary phase (Figure 16) after 90 mins; the mass is predominantly isointense to the adjacent liver parenchyma with few areas of hypointensity. No significant restricted diffusion with ADC drop was seen. The ADC value in the degenerated and non-degenerate areas was in the rang of 1.4 - 1.5 x10-3mm2/s.
The mass was diagnosed as Sclerosing haemangioma on the MRI and follow up interval imaging was recommended.
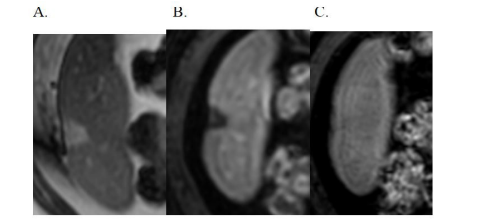
After three months patient came for a followup ultrasound which showed no change in the size of the hyperechoic mass in the right lobe (Figure 17A and B) with no other additional new observations.
Hepatic haemangiomas are benign group of focal lesions in the liver with a prevalence of ~20% [1]. Haemangiomas are most common incidentally detected lesions which are most of the times asymptomatic with relatively low rate of complications [2]. The role of imaging is important to diagnose these benign focal hepatic lesions.
MRI because of its high soft tissue resolution has become the modality of choice in diagnosing focal hepatic lesions with a high sensitivity and specificity of 98% [3].
However not all the hemangiomas have typical imaging features and thus it is important to identify the atypical haemangiomas which require only surveillance without any active interventions when asymptomatic
Typically hemangiomas less than 4cms show peripheral nodular enhancement with centripetal filling in of the intravenous contrast on the venous and delayed images.On the hepatobiliary phase these are predominantly hypointense [4]. Flash hemangiomas are smaller in size with enhancement on arterio portal phase and isointense on the venous and delayed images. Larger hemangiomas ,greater than 4 cms in size are giant hemangiomas which need intervention due to the risk of haemorrhage [5].
Other types of hemangiomas are calcified, cystic and pedunculated haemangioma. Sclerosing hemangiomas are rare focal hepatic lesions with varied imaging patterns due to degenerative changes such as extensive fibrosis, hyalinisation, obliteration of the vascular spaces, haemorrhage or sclerosis [6,7].
Hemangiomas are easily diagnosed on the Computed Tomography (CT) with triple phase contrast study, however due to heterogenous patterns sclerosing hemangioma requires high soft tissue resolution, MRI with its high soft tissue resolution helps in narrowing the differential diagnosis and further help in appropriate treatment plan for the patients. The DWI(Diffusion images and the ADC maps) help in differentiating benign from malignant hepatic tumours.The ADC values of malignant tumours like hepatocellular carcinoma, metastases, ICC, and hemangiomas were 1.15 ± 0.21 × 10−3, 1.23 ± 0.32 × 10−3, 1.52 ± 0.26 × 10−3, and 2.09 ± 0.43 × 10−3 mm2/s, respectively [8]. Contrast enhanced MRI further can be helpful in narrowing the differentials.
Geographic pattern, capsular retraction, reduction in the size on follow up and loss of previously enhancing areas suggest sclerosing haemangioma ; this was reported by Doyle et al [9]. However this is applicable when previous images are available.
Further PET CT is not very useful in this benign mass which are not FDG avid [10]. Our patients had no previous imaging details.The mass on MRI was hyperintense on the T2WI, against the predominant feature of sclerosing haemangiomas which are hypointense on the T2WI.
Sclerosing hemangiomas are rare benign focal hepatic lesions which involute over a period of time, however active interventions are needed when symptomatic.Imaging patterns are varied and inconclusive.

![]()

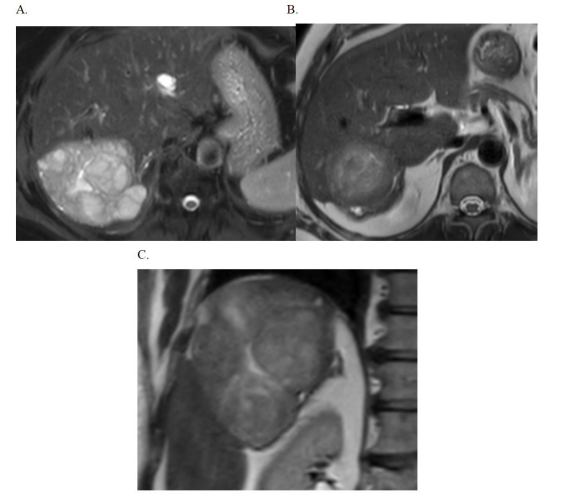 |
| Figure 1: A, B and C: Axial and coronal T2WI show lobulated observation in segment VII and VI with heterogenous appearance |
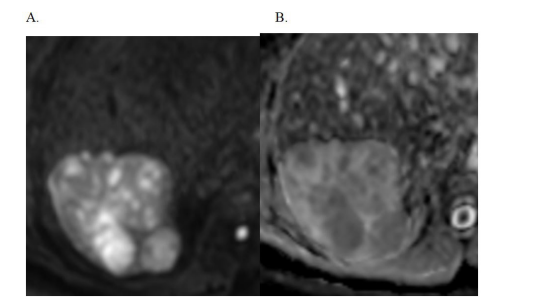 |
| Figure 2: A and B: Axial Diffusion weighted images and ADC showing heterogenous restriction |
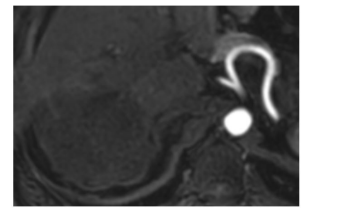 |
| Figure 3: Arterial Phase: No significant enhancement seen |
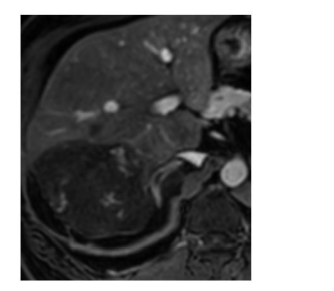 |
| Figure 4: Portal Phase: Focal central areas of enhancement |
 |
| Figure 5: Venous Phase: Very mild Heterogeneous enhancement |
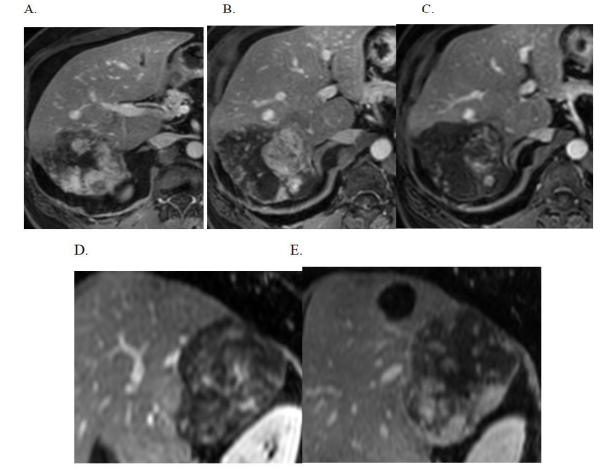 |
| Figure 6: (A, B, C, D and E) Delayed phase axial and sagittal images: Areas of heterogeneous enhancement with areas of non-enhancement |
 |
| Figure 7 A and B: Hepatobiliary phase: Areas of hypo and hyperintensity |
 |
| Figure 8A, B and C: Axial T2WI, Axial Delayed and Axial Hepatobiliary Phase Smaller segment VI focal lesion |
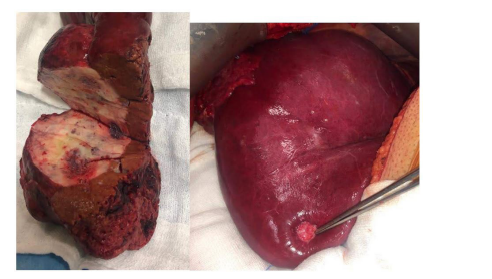 |
| Figure 9A and B: Surgical specimen(Larger lesion and smaller lesion in segment VI)Shows a hepatic solitary tumor which is well demarcated from hepatic parenchyma.The tumor is solid to spongy, fibrotic with patchy hemorrhagic areas |
 |
| Figure 10(A,B and C): Histopathology slides show tumor composed of many cavernous thin walled vascular interconnecting channels .The supporting stroma shows hyalinized sclerosis with fibroblasts. Vascular channels filled with blood |
 |
| Figure 11A and B: T2WI axial and coronal image shows a heterogenous well defined mass in the right lobe |
 |
| Figure 12: T1WI Axial image shows the mass to be predominanalty hyperintense with central hypointensity |
 |
| Figure 13: Axial arterial phase shows few foci of enhancement |
 |
| Figure 14: Axial portal phase shows heterogeneous enhancement |
 |
| Figure 15: Axial venous phase shows continued heterogeneous enhancement |
 |
| Figure 16: Axial hepatobiliary phase shows the mass as isointense to the adjacent liver parenchyma with areas of central hypointensities |
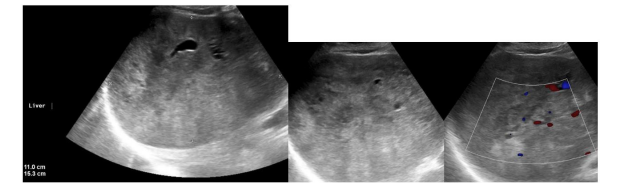 |
| Figure 17A and B: Follow up three months USG showed predominantly hyperechoic mass in the right lobe with no significant interval change in the size |




































