Open Access
Research Article
Max Screen
ISSN: 2456-5504
Copyright: © 2021 Mankar D. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Objectives:This study aims at describing the CT imaging findings and role of multidetector computed tomography (MDCT) in evaluation of squamous cell carcinoma of buccal mucosa and its staging. The imaging findings in squamous cell carcinoma (SCC) of the oral cavity allow the radiologist to accurately determine the extent and staging of disease thereby help clinicians plan appropriate treatment.
Materials and Methods:Retrospective study of 40 patients who underwent MDCT and were histopathogically proven case of squamous cell carcinoma (SCC) of buccal mucosa patients were included in the study. Plain, arterial, venous phase and puff cheek CT cuts were taken from base of skull till clavicle. All the CT imaging scans were performed on CT Philips machine (64 slices).
Results:We present CT imaging characteristics of 40 histopathogically proven case of squamous cell carcinoma (SCC) of buccal mucosa. Retrospective study of 40 such patients was done in which majority of them are male patients (27) as compared to female patients (13). Among these 40 patients, 20 patients had stage IVB cancer, 13 patients had stage IVA, 5 patients had stage II and 2 patients had stage I cancer. No patient included in our study had stage III.
Conclusions:MDCT is non-invasive and cost-effective investigation which helps in evaluating squamous cell carcinoma of buccal mucosa and determines its stage accurately. Patient’s recovery will depend on how early the cancer is found and staging gives an idea of patients’ possible outcomes.
Keywords: MDCT Buccal Mucosa; TNM Staging; Retromolar Trigone; Masticator Space; Lymph Nodes
List of abbreviations:MDCT: Multidetector Computed Tomography; CT: Computed Tomography; SCC: Squamous Cell Carcinomas; RMT: Retromolar Trigone; TNM: Tumor (T), Nodes (N), metastases (M); NP: Nasopharynx; LP: Lateral Pterygoid Muscle; MP: Medial Pterygoid Muscle; R: Ramus of Mandible; M: Masseter Muscle; B: Buccal Space; R: Ramus of Mandible; MP: Medial Pterygoid Muscle; M: Masseter Muscle
Squamous cell carcinomas (SCC) constitute more than 90% of all oral cancer. Other malignant tumours of oral cavity can arise from the epithelium, connective tissue, minor salivary glands, lymphoid tissue, and melanocytes or metastasis from a distant tumour [1]. Most common site of oral cancer in Indian population is buccal mucosa [2].
In the developed countries, carcinoma buccal mucosa is relatively uncommon as compared to the Indian subcontinent. The high incidence of oral cancer in India is mainly because of common use of gutkha and betel quid chewing (with or without tobacco), which make its population to a higher risk of developing oral sub mucous fibrosis, a premalignant disease resulting in increased incidence of oral cancer especially in younger patients [2]. Buccal mucosa is the inner lining / mucosal surface of cheek and lips. It is continuous with the buccal aspect of the gingiva of the maxillary and mandibular alveolar ridge, as well as the retro molar trigone.
Areca-nut/betel-leaf/tobacco chewing habits, tooth extraction, heavy alcohol use, sexually transmitted virus called human papillomavirus (HPV), Candidiasis, premalignant lesions like leukoplakia, erythroplakia and oral sub mucosal fibrosis.
Cross-sectional imaging plays a crucial role in the pre-operative evaluation of buccal mucosa cancer and provides precise details of the extent of lesion which can help decide the management and indicate prognosis. MDCT (multidetector computed tomography) is an easily available modality for evaluation of such cases. It is non-invasive and cost-effective investigation which helps in evaluating squamous cell carcinoma of buccal mucosa and determines its stage. Imaging features that affect staging and treatment planning like involvement of RMT, muscles of tongue, masticator space, bone and neurovascular bundle involvement and lymph nodal and distant metastasis are accurately provided by MDCT. Puffed cheek CT is an easy to perform technique and provides a clear and more detailed evaluation of buccal and gingival mucosa of oral cavity.
Current study aims at describing the CT imaging findings and role of multidetector computed tomography (MDCT) in evaluation of squamous cell carcinoma of buccal mucosa and its staging. The imaging findings in squamous cell carcinoma (SCC) of the oral cavity allow the radiologist to accurately determine the extent of disease and help clinicians plan appropriate treatment. Additional aim is to establish the relation between RMT (retromolar trigone) and tongue involvement.
Retrospective study of 40 patients who underwent MDCT and were histopathogically proven cases of squamous cell carcinoma of buccal mucosa was done.
Patients who were histopathogically proven cases and underwent imaging later and patients who already undergone imaging followed by biopsy and histopathological confirmation were included in the study
Plain, arterial, venous phases and puff cheek CT axial cuts were taken from base of skull till clavicle. Multiplanar sagittal & coronal reformatted images were obtained using multiplanar imaging. All the CT imaging scans were performed on CT Philips machine (64 slices). “Puffed-Cheek” technique was performed to improve visualization of superior and inferior gingivobuccal sulcus and RMT (retromolar trigone).
The staging was done with TNM classification.
• All the patients referred to radiology department for CT imaging and were histopathological proven cases of squamous cell carcinoma of buccal mucosa (before or after imaging).
• Time interval between patient who underwent biopsy first and later imaging or patients who already undergone imaging followed by biopsy and histopathological confirmation— less than 30 days.
• Post op case of buccal mucosa cancer
• Patients who have taken chemotherapy/radiotherapy for buccal mucosa cancer
• Recurrence of buccal mucosa cancer.
• Time interval more than one month between histopathological confirmation and CT scan.
In present study, there were a greater number of male patients (n=27) as compared to female patients (n=13). The range of age varied from 31 years to 70 years with equal distribution in age groups: 31-40 years (n=10), 41-50 years (n=10), 51-60 years (n=10) and 61- 70 years (n=10) as shown in figure 1. 85% of total patients had history of tobacco/areca nut/ betel nut chewing. 5% had history of smoking and 5% had history of oral infections while 5% of patients had no history of any addictions/ risk factors (Figure 1).
Among 40 patients, majority of them (20 patients - 50%) were classified as stage IVB with extension into masticator space. It was followed by stage IVA (13 patients - 32.5 %), stage II (5 patients - 12.5%) and stage I (2 patients - 4%). No patient having stage III cancer was found in this study (Figure 2).
Out of all patients, 2 patients (5%) had less than 2 cm size lesion, 21 patients (52%) had size in the range of 2-4 cm and 17 patients (43%) had size more than 4 cm.
RMT (retromolar trigone):22 patients out of 40 (55%) had extension into retromolar trigone. Majority of such patients had stage IV B cancer (81%). Others had stage II (9%) and stage IVA (9%).
Extrinsic and intrinsic muscles of tongue:8 patients (20%) with buccal mucosa cancer had extension into extrinsic and intrinsic muscles of tongue. RMT and tongue both were involved in 6 patients (15%).
Masticator space:20 patients (50%) had extension into masticator space with involvement of masticator muscles. Most of the cases had simultaneous involvement of two or more muscles. Masseter muscle was the most commonly involved muscle (17 patients42.5%), followed by medial pterygoid muscle (10 patients- 25%), lateral pterygoid muscle (7 patients- 17.5%) and temporalis muscle (6 patients- 15%).
Bone:23 patients (57.5%) had bone involvement (mandible/maxilla/pterygoid plates). Out of these 23 patients, only mandible was involved in 12 patients (52%), maxilla was involved in 8 patients (35%) and mandible, maxilla and pterygoid plates all three were involved in 3 patients (13%).
Perineural spread:5 patients (12.5%) had extension in mental foramen and mandibular canal with its widening and destruction, s/o perineural spread.
Maxillary sinus:6 patients (15%) had extension into maxillary sinus.
Skin: 16 patients (40%) had involvement skin with its thickening and ulcer formation.
Lymph nodes:29 patients (72.5%) had regional lymph nodal metastasis. Of these, 20 patients (69%) had ipsilateral lymph nodal involvement while 9 patients (31%) had bilateral lymph nodal involvement.
Distant metastasis:No patient had any distant metastasis.
MDCT helps in detecting the primary lesion, its extension and thus, helps in staging the disease.
On MDCT imaging buccal mucosa cancer can be seen as- Plaque like thickening, irregular fungating or ulcero-proliferative growth. Complicated cases can show orocutaneous fistula.
Primary buccal mucosa malignancies rarely metastasize to distant sites. They usually metastasize to lymph nodes or spread locally. It usually spreads by three general ways: (a) by direct extension (b) by dissemination via lymphatic drainage pathways, and (c) by extension along neurovascular bundles. For accurate staging of SCCs of the buccal mucosa, evaluation of these three routes of spread is mandatory [3].
Important structures to look for while describing buccal mucosa cancer and its extension on MDCT are as follows:
• Buccal mucosa- buccinator complex.
• Buccal space.
• Superior and inferior gingiva-buccal mucosa.
• Retromolar trigone.
• Pterygoid muscles.
• Masseter muscle
• Mandibular bone involvement and residual height.
• Mandibular canal/ perineural spread.
• Parotid duct involvement.
• Cervical lymph nodes.
There are different staging systems but most commonly used is TNM system.
The involvement of retromolar trigone is one of the common patterns of extension found in our study besides ipsilateral lymph nodes and bone. The commonest imaging extent of the tumour was noted as stage IVB within one month of histopathological diagnosis in our study suggesting aggressive spread of buccal carcinoma. Thus, the real extent of these tumours is maybe underestimated at first clinical examination. Secondly the onset of symptoms that is noticed by the patient, the tumour may already have a widespread local extension.
The different stages of cancer describe how far the cancer has grown and spread at the time of diagnosis. An early-stage cancer may call for surgery while an advanced-stage cancer may need chemotherapy.
Factors which influence a particular surgical approach are size of lesion, its proximity to bone and depth of infiltration. Reconstruction of major surgical defects in the oral cavity requires use of a free flap. Mandibular sparing surgeries like marginal mandibulectomy and mandibulotomy are popular with no, or minimal, cortical mandibular invasion. At least, a 1-cm thick segment of bone must be left inferiorly after a marginal mandibulectomy. Marginal mandibulectomy is contraindicated in patients with gross clinical and radiological involvement of mandible, invasion of mandibular canal by cancer and in deeply infiltrating lesions of gingivobuccal sulcus where there is paramandibular infiltration, as the margin of resection may pass through infiltrated paramandibular tissue [4].
Early lesions (T1–T2) can be effectively treated with either surgery or radiation as single modality. Advanced lesions require multimodality treatment with surgery, adjuvant radiotherapy or chemotherapy [5].
CT images of few patients are as followed with their corresponding TNM staging
A 36 year old female complaining of ulcerative growth in inner aspect of right cheek since 3 months. She had history of tobacco chewing since 10 years. She denied other addictions. No co-morbidities were present.
A 48 year old lady came with complaints of ulcer over right cheek since 20 days. No h/o discharge
She had history of tobacco chewing for 12 years. No co morbidities were present.
A 53 year old male c/o swelling on right side of face and decreased opening of mouth since 3 months. H/o tobacco chewing for 12 years. No co-morbidities present.
A 70 year old male c/o swelling and ulcer on left side of face. H/o tobacco chewing for 20 years. On medication for diabetes since 10 years. No other co-morbidities present.
MDCT is non-invasive and cost-effective investigation which helps in evaluating squamous cell carcinoma of buccal mucosa and determines its stage. Patients recovery will depend on how early the cancer is found and staging gives an idea of patient`s possible outcomes. Imaging features that affect staging and treatment planning like involvement of RMT, muscles of tongue, masticator space, bone and neurovascular bundle involvement and lymph nodal and distant metastasis are accurately provided by MDCT. MDCT helps in determining the extent of bone involvement and gives an idea about the outcome of mandible sparing surgery like marginal mandibulectomy.

![]()

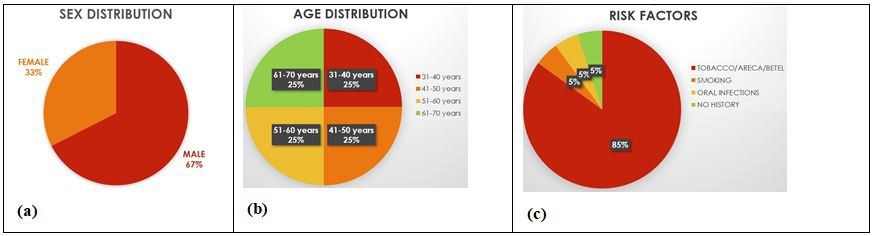 |
| Figure 1: Distribution of patients according to sex (a), age (b) & risk factors (c) |
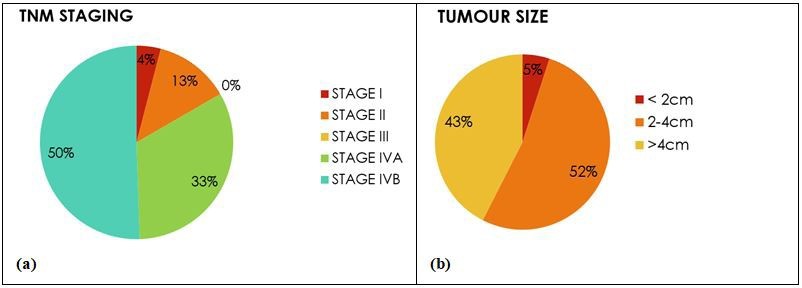 |
| Figure 2: Pie chart depicting TNM staging wise distribution of patients (a) and tumour size distribution (b) |
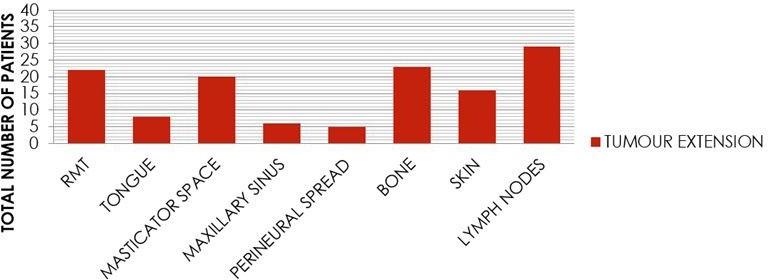 |
| Figure 3: : Column bar diagram depicting extension of primary tumour in RMT, tongue muscles, masticator space, maxillary sinus, perineural, bone, skin and lymph nodes |
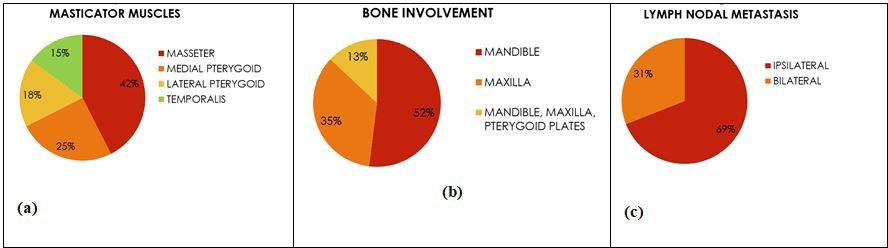 |
| Figure 4: Pie chart depicting extent of tumour in different muscles of masticator space (a) bones; (b) and lymph nodes (c) |
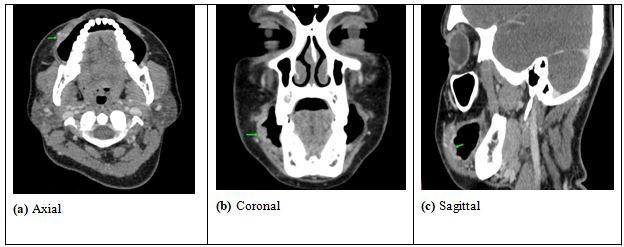 |
| Figure 5: In this histopathology proven case of SCC of right buccal mucosa, (a) Axial; (b) Coronal and (c) Sagittal shows mildly enhancing plaque
like ulcerative soft tissue density lesion involving the right buccal mucosa buccinator complex. No extension into retro molar trigone noted TNM staging:T1 tumour - less than 2 cm in size, N0 - no regional lymph nodes involved, M0- no distant metastasis - Stage I cancer. |
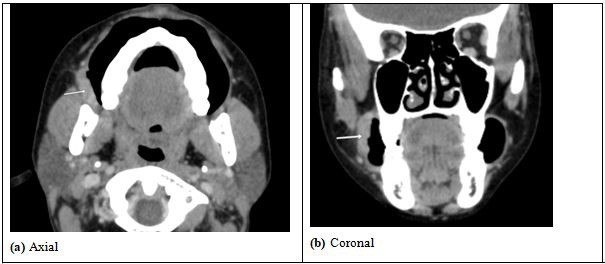 |
| Figure 6: Heterogeneously enhancing plaque like ulcero-proliferative soft tissue density lesion measuring < 4cm in greatest dimension noted in right
buccal mucosa-buccinator complex involving the superior gingivobuccal sulcus extending into the retromolar trigone (a and b) TNM stagingT2 - tumour is more than 2 cm but less than 4 cm, N0 - no nodal involvement, M0- no distant metastasis - Stage II cancer. |
 |
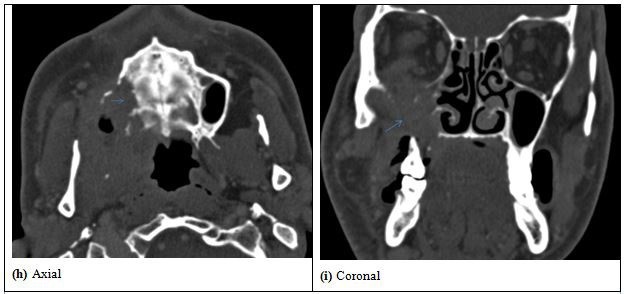
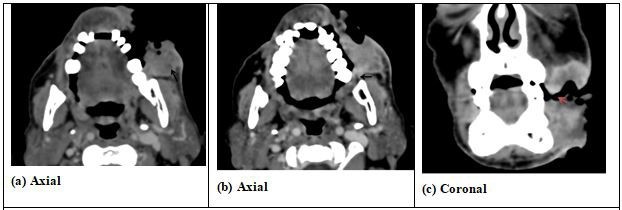
| Figure 7: (a) An ill-defined heterogeneously enhancing ulcero-proliferative growth noted involving right buccal
mucosa-buccinator complex (black arrows) and right retromolar trigone (blue asterix) (b) The major part of the lesion is in infratemporal region, maxillary region, retromaxillary space and involves maxillary sinus with destruction of the right maxillary sinus walls |
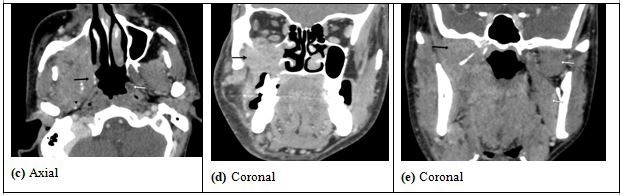 |
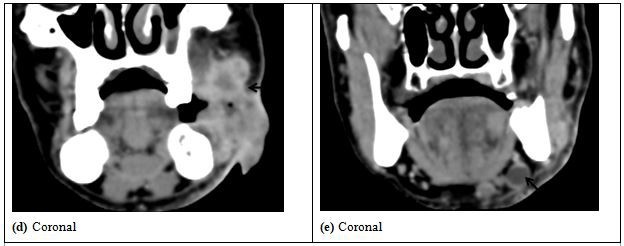
| Figure 8: (c) The lesion is extending to involve the right lateral wall of nasopharynx with obliteration of Eustachian tube and fossa of Rosen Muller (black arrows).
Compare with normal left lateral wall of nasopharynx (white arrows) (d) Bony erosion of the right side of hard palate and erosion of floor of right orbit with intra-orbital extra-conal extension abutting the inferior rectus muscle and inferior oblique (e) In the infra-temporal fossa there is involvement the right medial pterygoid and lateral pterygoid muscles (black arrow). Normal left medial pterygoid and lateral pterygoid muscle (white arrows) |
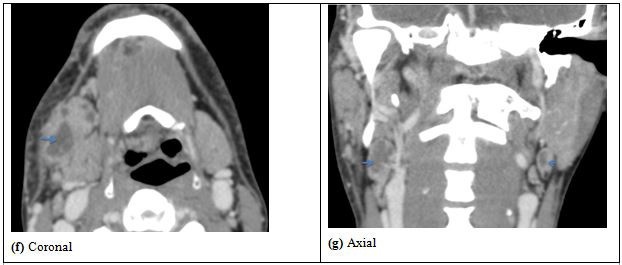 |
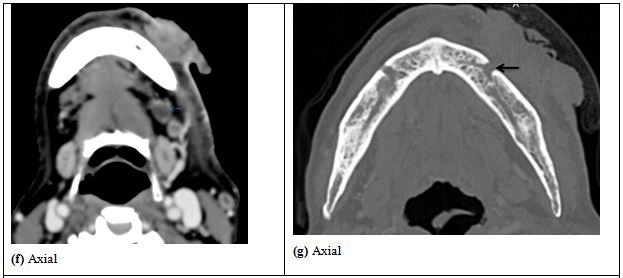
| Figure 9: Multiple discrete and conglomerate necrotic lymph nodes noted in right level Ib (f) and bilateral levels II (g), and is abutting the right submandibular gland with loss of fat planes |
 |
| Figure 10: Bony erosion of the right side of hard palate and erosion of floor of right orbit with intra-orbital extra-conal extension abutting the inferior rectus muscle and inferior oblique muscle |
 |
| Figure 11: (j and k)Bony erosion of right pterygoid processes of sphenoid bone TNM staging:: T4b tumour - primary tumour involves cortical bone, pterygoid plates, maxillary sinus and masticator space; N2c - Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension; M0- no distant metastasis - Stage IVB cancer |
 |
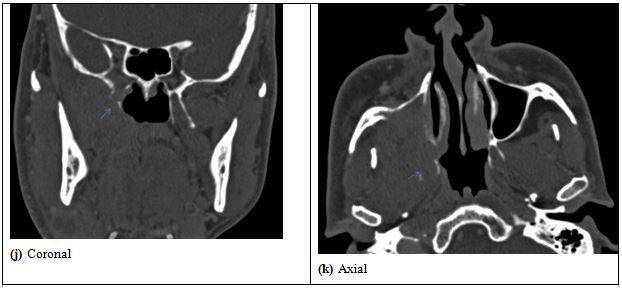
| Figure 12: An ill-defined heterogeneously enhancing ulceroproliferative soft tissue density lesion involving left buccal mucosa - buccinator complex. The lesion is seen reaching upto the overlying skin with its thickening and causing ulceration of the skin with a large defect suggestive of orocutaneous fistula (a and c); The lesion also extends minimally into the left retromolar trigone (b) |
 |
| Figure 13: The lesion is involving superior and inferior gingivobuccal sulcus |
 |
| Figure 14: (f) Multiple mildly enlarged discrete heterogeneously enhancing lymph nodes seen in level Ia (not shown) and left level Ib (e and f)
(g) Mild widening of left mental foramen seen s/o perineural spread TNM staging: T4a tumour - primary tumour involves skin and perineural spread, N2b - Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension, M0- no distant metastasis - Stage IVA cancer. |
T-Tumour: |
|
|
|
|
|
|
|
|
Note that Tx, T0, and Ti tumours are not radiologically visible. |
N-Lymph Nodes (regional metastasis): |
|
|
|
|
|
|
|
M-Metastasis: |
|
|
Stage |
|
TNM staging |
Criteria |
|
|
|
|
I |
T1N0M0 |
Tumour less than 2cm |
|
II |
T2N0M0 |
Tumour more than 2cm but less than 4cm |
|
III |
T3N0M0 or T1/T2/T3- N1 M0 |
Tumour > 4cm or ipsilateral node < 3cm |
|
IV |
IV A |
T1/T2/T3 –N2 M0 or T4a- N0/N1/N2 M0 |
All N2 lesions. Invasive lesions involving cortical bone, intrinsic or extrinsic muscles of the tongue, maxillary sinus, or skin. |
IV B |
T1/T2/T3- N3 M0 or T4b – N1/N2/N3 M0 |
All N3 lesions. Invasive lesions infiltrating masticator space, pterygoid plates, skull base or encase the carotid artery. |
|
IV C |
T1/T2/T3/ N1/N2/N3 - M1 |
All M1 lesions (distant metastasis). |
|





































