Open Access
Research Article
Max Screen
ISSN: 2456-5504
Copyright: © 2020 Woodard S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Teamwork has been a recent focus of radiology literature on multidisciplinary and intradepartmental levels. Several publications discuss team building roles and daily checklist utilization. The overall endpoints of these studies vary; however, the theme is to improve workflow, patient safety, problem-solving, and department morale. In this single institution study conducted within our academic medical center breast imaging section, we sought to assess team confidence in daily operations and staffing by evaluating survey responses before and after the implementation of morning team huddles. The goals of the study are to assess trends and statistical significance in survey responses regarding daily workflow and gauge the overall utility of team huddles in improving perceived knowledge of staffing and scheduling at the beginning of each day. We recognize that with the onset of COVID-19, many changes have been made regarding social distancing; however, this study was performed prior to the pandemic and will be increasingly relevant with the return to normal workflow.
Keywords: Breast; Radiology; Teamwork; Workflow; Huddle; Preparedness
Several investigators have studied the dynamic of a team environment in academic radiology. Weinreb discussed the idea of teamwork in academic radiology and its importance in the roles of leadership and support staff. This article addressed the role of trust in teamwork and the positive effects of group dynamics when teams are implemented. It emphasized the importance of motivation and cooperation. While the focus of this article was creation of general team for an entire department, the concepts hold true for specific radiology sections [1].
In 2010, Lane Donnelly et al. discussed the importance of communication and teamwork in improving patient safety. They designed a project around the concepts of horizontal and vertical interventions (horizontal being culturally and environmentally caused errors versus vertical involving actual errors themselves). They evaluated baseline safety performance with a two year follow up that showed decrease in the serious safety events reported (one per 200 days versus one per 839 days). This was considered statistically significant [2].
Donnelly then went on to publish an article in 2017 on the current problems in diagnostic radiology. In this paper, a ‘daily readiness huddle’ was implemented composed of a small group of people. These groups discussed metrics, created displays and electronic summaries, and outlined various group goals. This program was not only conducted at the radiology department level, but it was implemented throughout multiple radiology sections as well. The overall assessment from this project was that such a process allowed the team to better identify problematic issues, create solutions, and create camaraderie between physicians and staff [3].
Spraygun et al. looked at teamwork with respect to expenses and improving service. They implemented a one-year program that showed improvement in measurable outcomes [4]. In 2018, Hannah et al. looked specifically at the S Mesa model (Safety, Methods, Equipment, Supplies, and Associates) when they composed a survey regarding daily (or slightly less frequent) huddles. They evaluated multiple aspects of huddles including radiologist preferences. This was a very broad group of participants ranging from the highest number of participants in pediatric neuroradiology and lowest in urban head and neck imaging. Data was collected using a Likert scale within Emory Healthcare Radiology. The huddles were typically five minutes or less and were designed to improve communication, add structure, review tasks, problem solve/manage/evaluate, and improve collaboration. Regarding the design of huddles, some of the participant comments were unfavorable citing that the meetings contained unnecessary information specifically regarding staff coverage when there are few assignments in certain radiology sections. The favorable comments pointed out that certain rotations that involve procedures and multiple attendings are most in need of team huddles. In addition, the presence of fellows and residents was felt to warrant huddling. No baseline data was collected in the study and the impact on patient care was not evaluated [5]. These comments are particularly relevant to our breast imaging section, which involves multiple daily assignments for both radiologist and technologist while also requiring integration of undergraduate students, medical students, residents, and fellows.
As a quality improvement project, this study was determined to be exempt from institutional review board review. At our institution in the breast imaging section of the department of radiology, we underwent significant change in staffing from radiologists, administrative support staff, patient care coordinators, and technologists from 2017 to 2019. In an effort to improve familiarity, daily workflow knowledge, and clarity of schedule, daily team huddles were implemented in August 2019. A modified Likert scale (0 to 10, zero being least confident and 10 being most confident) baseline survey was administered to all voluntary participants including radiologists, administrative staff, patient coordinators, and technologist. These surveys were anonymous and included six questions (Figure 1). Survey questions assessed the confidence of each participant regarding their specific individual role in workflow, the assignment of all technologists and breast imaging radiologists every day (technologist and radiologist roles typically change daily whereas administrative support staff and patient care coordinators typically do not change roles), the daily procedures, equipment issues, and rotating residents/medical students.
A lead technologist role had recently been created and defined. The lead technologist conducted the team huddle every day. The outline for each huddle (Figure 2) specified the following: a greeting, remind of any special occasions either internal or external to the section, identification of team members (technologist, breast imaging radiologist, radiology residents, medical students, staff), equipment issues or scheduled maintenance, special reminders (vendors, site visits, news), and a comical or inspirational quote of the day. These team huddles were designed to be approximately five minutes in duration and were conducted for six months. At the end of the six-month period of time, a second survey was conducted with the exact same questions using the same modified Likert scale from 0 to 10. All collected surveys were anonymous and data was subsequently compiled. Descriptive analysis and two -group Mann-Whitney test U-test was used to compare baseline and after survey score from two groups of anonymous participants. Although the roles (radiologist, administrative staff, patient coordinator, and technologist) of the participants were the same, the participants, themselves, were anonymous volunteers. One new technologist hire had joined the section since the initial survey, and it is unknown whether or not that hire participated in the follow-up survey.
A total of 21 participants filled out the baseline survey (Table 1). Mean scores ranged from 5-9. Questions resulting in the lowest overall scores were those involving equipment issues and residents/medical students on the breast imaging rotation. These both averaged a five on the modified Likert scale. The higher scored questions were those involving the specific individual’s role in workflow as well as the radiologists’ role in workflow, both averaging 9 on the modified Likert scale.
The follow-up survey was also anonymous with a total of 15 participants (Table 2) conducted in January of 2020. Mean scores range from 8-10. Lowest scored categories included the procedure and equipment categories, both resulting in a mean score of eight on the modified Likert scale. The highest categories involved the technologists’ and radiologists’ role in workflow each day, similar to the baseline survey.
The mean values from each question on the baseline and follow up surveys are compared in Table 3. Each average value for the 6 questions demonstrated an overall increasing mean from baseline to follow-up survey. Figures 3 and 4 demonstrate specific data points plotted on a bar graph, illustrating progressive trends toward a decrease in the number of participants choosing lower scores and increase in the number of participants choosing higher scores from baseline to follow-up survey.
Table 3 presents the change between baseline and follow-up surveys. While overall trends can be noted in the data points, there were statistically significant improvements in certain questions, specifically questions 2, 5, and 6. These questions included the following: Do you know who/where (technologist) is scheduled to work each day (breast imaging)? Do you know of equipment issues at the start of each day? Are you confident that you can identify the residents/med students on this breast imaging rotation? Although we saw the trend of improvement from all questions in survey 2 compared to survey 1, the statistically significant improvement is seen in questions 2 (Q2, p = 0.0070), 5 (Q5, p = 0.0367), and 6 (Q6, p = 0.0096) with average of score increase (between two scores) of 2.81, 2.79 and 3.50 respectively using two-group Mann-Whitney test U-test.
Numerous radiology groups have investigated the benefit of having a group huddle to promote increased communication, morale, and teamwork, including the studies described above from Weinreb, Donnelly, Spraygun, Hannah, and colleagues. In breast imaging especially, the importance of open communication is highlighted by the daily interactions involved in running a clinic. Various types of patient encounters, ranging from screening exams, diagnostic evaluation, biopsy procedures, localization procedures in coordination with same-day subsequent surgeries, and pathology follow-up occur daily in breast imaging. Each of these processes requires multiple interactions between patient coordinators, technologists, staff, medical students, residents, fellows, radiologists and patients. Organization between these groups is imperative.
In our breast imaging section, a significant turnover of personnel had recently taken place and as a result, gaps in communication, workflow knowledge, and general functioning of the section became evident. A baseline survey evaluating general confidence levels regarding fluctuating team member roles was administered to various team members. Areas of strength and weakness were identified from survey questions. Previous work from other authors and reported success of team meetings guided the implementation of these morning huddles.
Our huddles were designed to be both an opportunity for an introduction of new faces (medical students, residents, undergraduates, rotating or visiting learners, and new hires) and an opportunity for identification of issues that may impact workflow. As there were comments in prior studies such as Spraygun et al. that criticized huddles as being intrusive, ours were designed to take place at the least busy time of the day, last only five minutes in duration, and be as succinct as possible. While attendance was not mandatory, the huddle was announced clearly throughout the section every morning and all were invited to attend. Unless otherwise involved in a case, we generally had all team members participating in the meeting.
We found that there were statistically significant improvements in the scored responses regarding scheduling of technologist, identification of residents and medical students on the rotation, and the equipment issues within the section. Although the remainder of the questions did not show a statistically significant improvement, a clear trend of improved overall scores can be seen.
Each question was designed to assess the confidence and knowledge of the specific team member regarding the roles of those who consistently have distinct assignments on different days. In our section, technologists, radiologist, residents, medical students, and fellows are all assigned different roles day-to-day. For administrative staff and patient care coordinators, being knowledgeable of the daily clinical roles at the start of the day helps to direct patients and clinicians to the appropriate team member. Undergraduate, graduate, and medical students all rotate through the breast imaging section and may be scheduled random days or weeks at a time. For these learners, the huddle provides an introduction, a brief overview of daily activities, general layout of scheduling, and a welcome into a friendly environment. Residents spend approximately one month on the rotation but change assignments on a weekly basis, working with different attendings each day. Since this is a teaching institution, cases are first brought to the resident. The huddle allows technologists to be aware of these assignments and collaborate with the appropriate resident prior to presenting the case to his/her attending. Fellows have a similar arrangement with weekly assignments. Technologist are assigned to different positions, ranging from biopsies to screening. These positions also change based on morning and afternoon shifts. It is beneficial for each team within the section to identify its members.
Although other studies have examined specific opinions and feelings on team huddles, this particular study did not question the opinion of the participants. A follow-up study could potentially investigate the willingness of participants to continue with team huddles. Despite no formal process of evaluating the overall satisfaction of team huddles, general consensus from our staff, technologist, and radiologist interaction was that the huddles were a positive experience and provided an overall boost in morale.
One limit of this study was lack of an actual attendance record. It is unknown which respondents participated in the fewest or the most huddle sessions and how this information may have impacted the results of the study. As previously mentioned, one additional technologist had been hired since beginning huddles and it is unknown if this hire participated in the follow-up survey. Another limit is the distribution of survey participants. The respondents ranged from radiologists and technologists, to patient coordinators and administrative staff. This likely had an impact on general knowledge of workflow. The final limitation of the study is compounding factors that involve all work environments, such as staff fluctuation and minor variations in scheduling
Overall, we found team huddles to be a positive experience, showing a statistically significant improvement in scored responses regarding scheduling of technologists, identification of residents and medical students on the rotation, and equipment issues within the section. We also saw a general trend toward improved scores involving all questions. Questions not demonstrating statistically significant improvement are those involving the individual’s own role, the radiologist’s role, and the procedures planned for the day. These aspects of scheduling could be emphasized in future huddles to better inform the team and improve all aspects of daily workflow preparation. The satisfaction of huddles and opinions of the faculty and staff were not measured; however, there were positive workroom comments regarding the overall welcoming environment that team huddles provided. This supports prior studies that have reported similar experiences. In conclusion, succinct, focused, and informative team huddles are beneficial to workflow confidence in breast imaging and should be considered for improving team preparedness and communication.

![]()

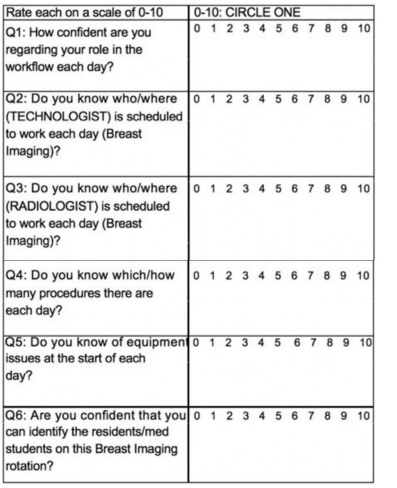 |
| Figure 1: Survey |
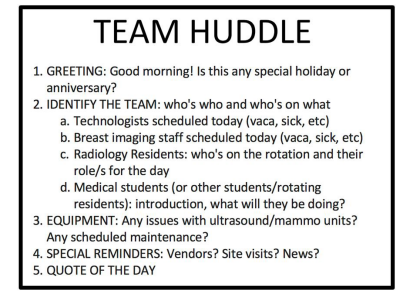 |
| Figure 2: Huddle outline |
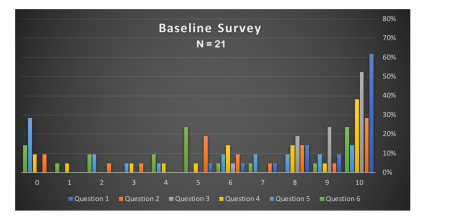 |
| Figure 3: Data plots from baseline survey with questions 1-6 showing scores ranging from 0-10 |
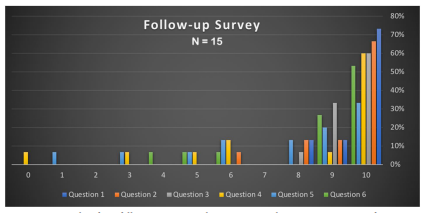 |
| Figure 4: Data plots from follow-up survey with questions 1-6 showing scores ranging from 0-10 |
|
Q1 |
Q2 |
Q3 |
Q4 |
Q5 |
Q6 |
Participant 1 |
9 |
5 |
9 |
6 |
2 |
2 |
Participant 2 |
10 |
10 |
6 |
6 |
0 |
0 |
Participant 3 |
7 |
0 |
10 |
1 |
0 |
10 |
Participant 4 |
10 |
6 |
9 |
5 |
2 |
10 |
Participant 5 |
10 |
10 |
10 |
10 |
4 |
2 |
Participant 6 |
10 |
3 |
10 |
6 |
8 |
1 |
Participant 7 |
10 |
10 |
10 |
0 |
0 |
0 |
Participant 8 |
10 |
5 |
10 |
10 |
10 |
5 |
Participant 9 |
5 |
5 |
8 |
0 |
0 |
5 |
Participant 10 |
10 |
10 |
10 |
10 |
10 |
4 |
Participant 11 |
9 |
2 |
9 |
9 |
0 |
10 |
Participant 12 |
10 |
8 |
8 |
4 |
7 |
9 |
Participant 13 |
8 |
9 |
8 |
3 |
9 |
5 |
Participant 14 |
6 |
6 |
10 |
10 |
7 |
0 |
Participant 15 |
10 |
8 |
10 |
8 |
9 |
7 |
Participant 16 |
10 |
10 |
10 |
10 |
8 |
6 |
Participant 17 |
10 |
10 |
10 |
10 |
10 |
10 |
Participant 18 |
8 |
8 |
8 |
8 |
6 |
5 |
Participant 19 |
10 |
7 |
9 |
10 |
6 |
4 |
Participant 20 |
8 |
5 |
9 |
8 |
3 |
10 |
Participant 21 |
10 |
0 |
10 |
10 |
0 |
5 |
MEANS |
9 |
7 |
9 |
7 |
5 |
5 |
|
Q1 |
Q2 |
Q3 |
Q4 |
Q5 |
Q6 |
Participant 1 |
8 |
9 |
9 |
0 |
8 |
9 |
Participant 2 |
10 |
10 |
9 |
9 |
9 |
9 |
Participant 3 |
9 |
9 |
9 |
5 |
9 |
4 |
Participant 4 |
10 |
10 |
10 |
10 |
5 |
5 |
Participant 5 |
8 |
10 |
10 |
10 |
10 |
10 |
Participant 6 |
10 |
10 |
10 |
10 |
10 |
10 |
Participant 7 |
10 |
10 |
10 |
10 |
10 |
10 |
Participant 8 |
10 |
10 |
10 |
10 |
8 |
10 |
Participant 9 |
9 |
10 |
9 |
10 |
6 |
6 |
Participant 10 |
10 |
6 |
9 |
6 |
3 |
9 |
Participant 11 |
10 |
8 |
10 |
6 |
6 |
9 |
Participant 12 |
10 |
10 |
10 |
10 |
10 |
10 |
Participant 13 |
10 |
8 |
8 |
3 |
1 |
10 |
Participant 14 |
10 |
10 |
10 |
10 |
9 |
10 |
Participant 15 |
10 |
10 |
10 |
10 |
10 |
10 |
MEANS |
10 |
9 |
10 |
8 |
8 |
9 |
|
Survey 1 (N=21) |
Survey 2 (n=15) |
Difference (Survey 1-Survey 2) |
|||||||
|
Mean |
95% CL Mean |
Mean |
95% CL Mean |
Mean |
95% CL Mean |
P-value |
|||
Q1 |
9.0476 |
8.3652 |
9.73 |
9.6 |
9.192 |
10.008 |
-0.5224 |
-1.4065 |
0.3018 |
0.3539 |
Q2 |
6.5238 |
5.0375 |
8.0101 |
9.3333 |
8.6826 |
9.9841 |
-2.8095 |
-4.6064 |
-1.0127 |
0.007 |
Q3 |
9.1905 |
8.6998 |
9.6811 |
9.5333 |
9.1789 |
9.8877 |
-0.3429 |
-0.977 |
0.2913 |
0.4367 |
Q4 |
6.8571 |
5.2654 |
8.4489 |
7.9333 |
6.1639 |
9.7028 |
-1.0762 |
-3.3956 |
1.2432 |
0.2768 |
Q5 |
4.8095 |
3.0254 |
6.5936 |
7.6 |
6.0365 |
9.1635 |
-2.7905 |
-5.2018 |
-0.3792 |
0.0367 |
Q6 |
5.2381 |
3.6101 |
6.866 |
8.7333 |
7.6166 |
9.8501 |
-3.4952 |
-5.5789 |
-1.4116 |
0.0096 |




































