Open Access
Research Article
Max Screen
ISSN: 2456-5504
Copyright: © 2019 Gandhi A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Diaschisis refers to depression of neuronal activity in an area that is remote from a focal disturbance in the brain but is connected to it by white matter tracts. When the cerebellum is affected, it is referred to as crossed cerebellar diaschisis (CCD) and involves the corticopontine tracts. Although CCD has been classically described in stroke, it can also be a sequela of other conditions including tumours, encephalitis, cerebritis, and intracerebral haemorrhage. Herein, we describe a rare case of CCD in the setting of status epilepticus, explore underlying mechanisms and draw parallels with the more commonly seen stroke-induced CCD.
Keywords: Seizure Edema; Crossed Cerebellar Diaschisis; Cytotoxic Edema
List of abbreviations:RUE: Right Upper Extremity; LUE: Left Upper Extremity; EEG: Electroencephalogram; MRI: Magnetic Resonance Imaging; CCD: Crossed Cerebellar Diaschisis
A 77-year old female was found unresponsive, incontinent of urine and demonstrating left sided gaze and occasional twitching of her right upper extremity (RUE). She had no prior history of seizures and was taking medications for a schizoaffective disorder. Her outpatient medications were discontinued during the hospital stay. The patient was admitted to the neurointensive care unit with a Glasgow Coma Score of 9 due to spontaneous movements of the RUE and withdrawal to pain in the left upper extremity (LUE). An EEG revealed status epilepticus. Multiple lumbar punctures were negative for meningitis or encephalitis. She remained in status epilepticus for at least 9 hours as her seizures were refractory to treatment attempts. She was treated with phenobarbital, valproic acid, phenytoin and clonazepam. Lacosamide was also administered but was immediately discontinued due to development of bradycardia. Intravenous immunoglobulin and steroids were administered in order to exclude the possibility that the refractory seizures were due to autoimmune encephalitis but these measures proved unsuccessful and the patient persisted in status epilepticus. A brain MRI was performed approximately 18 hours after initial presentation. The patient’s overall condition declined rapidly and on day 13 of her hospitalization, the patient’s family decided to remove life-prolonging measures and the patient expired shortly thereafter.
MR imaging of the brain demonstrated restricted diffusion and abnormal gyriform FLAIR signal involving the left frontal lobe, affecting the cingulate, inferior and middle frontal gyri and the frontal operculum (Figure 1a and b). Coronal FLAIR sequences demonstrated additional areas of abnormal signal in the left anteromedial thalamus and portions of the striatum; these areas, unlike the left frontal cortex, did not demonstrate corresponding restricted diffusion (Figure 2). In addition to the left frontal cortex, restricted diffusion and bright signal on FLAIR were observed in the right cerebellum, affecting the tonsil, the cerebellar folia and inferior segments of the vermis, including the tuber, pyramis, and uvula (Figure 2 and 3). No pathologic enhancement was demonstrated. The cortical restricted diffusion was compatible with seizure edema and the contralateral cerebellar diffusion restriction was attributable to crossed cerebellar diaschisis caused by seizure edema.
The term “diaschisis” (from the Greek dia “in half ” or “across” and schizien “to split”) was introduced by von Monakow in 1914, describing the phenomenon as a loss of excitability distant from a focal brain lesion with associated loss of intervening connections. Over the next 50 years, the clinical impact of this interesting observation was reduced by its overutilization to rationalize numerous clinical presentations not readily attributable to a focal brain lesion. The overuse of crossed diaschisis to explain neurologic symptoms was in part due to a limited understanding of several physiologic mechanisms, including the behavior of neurons in the ischemic penumbra, for example. In the late 1970s, with the development of metabolic and perfusion imaging, there was a renewed interest in this topic. Areas of diaschisis were defined by decreased metabolism and/or cerebral blood flow, attributed to reduced neuronal and synaptic activity. This definition was based on the hypothesis that neurovascular coupling is preserved in areas of diaschisis. Recently, there have been several animal studies that suggest this may not always be the case. Specifically, areas of diaschisis as measured by perfusion seem to underestimate the extent determined by energy metabolism or neuronal activity. This suggests that perfusion may be preserved in areas of impaired metabolism and that there is a partial neurovascular decoupling [1].
Distinct types of diaschisis have been proposed. Focal diaschisis refers to the presence of remote circumscribed neurophysiological changes based on the classic understanding of diaschisis. Non-focal diaschisis relates to non-focal changes including changes in strength and direction of distant connections of a network [2].
CCD refers to a focal disturbance in the cerebellar hemisphere contralateral to the site of supratentorial injury. It has been widely described in the setting of stroke. Specifically, when there is decreased blood flow and oxygen to the cerebrum, there is parallel depression of the neuronal metabolism and activity depicted as reduced blood flow to the cerebellar hemisphere contralateral to the supratentorial pathology. This connection between the original and distant site is thought to involve the corticopontine tract which “exclusively projects to the contralateral cerebellum via the traverse pontine fibres and middle cerebral peduncles” [3]. Many cortical areas do not contribute to CCD. It appears that it is the location of the lesion, rather than its severity, which is the primary determinant of CCD [4].
Our case delves into a rare entity, CCD in the setting of seizure edema [5]. A wide variety of peri-ictal neuroimaging findings have been described in the literature. These findings can be described as local or remote, with respect to the site of seizure onset focus. Remote findings include posterior leukoencephalopathy, unilateral/bilateral diencephalic lesions, splenium abnormalities and CCD [6]. The pathophysiologic basis of lesions occurring remote from the site of ictal activity is poorly understood.
A few studies using multisequence MRI and MR spectroscopy have demonstrated diffusion abnormalities, increased lactate and decreased N-acetyl aspartate in the epileptogenic area in a pattern suggestive of cytotoxic edema [5,7]. Proposed mechanisms of cytotoxic edema include failure of Na+/K+-ATPase, excessive release of excitatory amino acids, and increased membrane permeability. The suspected presence of cytotoxic edema in the setting of status epilepticus is indirectly confirmed by the frequently observed presence of restricted diffusion seen on MRI in the affected cortex [7]. Restriction of Brownian water motion is a firmly established indicator of cell swelling due to severe and usually irreversible ischemic injury. Similar patterns of restricted diffusion have been described in cerebral cortex after prolonged episodes of status epilepticus and such observations lend support to the notion that seizure edema is likely, at least in part, attributable to a cytotoxic process leading to cell swelling. Additional studies have demonstrated that vasogenic edema also plays a role in the epileptogenic area, likely related to the breakdown of the bloodbrain-barrier and ictal hyper perfusion [7,8]. Irrespective of the diffusion changes in the ictal area, there is decreased afferent input to the contralateral cerebellum through the corticopontine fibres and consequent reduction in metabolism and cerebral blood flow. Oftentimes, including in our case, the thalamus may also be involved because it is thought to be a “relay station” connecting the tracts. Hence, the mechanism that might explain CCD induced by seizure edema is similar to the one postulated as the basis of CCD caused by cerebral infarcts. In essence, the common denominator in either setting is the presence of cytotoxic edema, whether it is caused by an ischemic insult or a prolonged seizure activity. In the setting of ischemia, the decreased flow of oxygenated blood to the cerebral cortex leads to Na+/K+ pump failure, alteration of cell membrane permeability, neuronal death and swelling and thus cytotoxic edema. Similarly, prolonged cortical excitation due to status epilepticus increases lactic acid and excitatory amino acids, decreases N-acetylaspartate in the affected cortex [5,7], leads to failure of Na+/K+-ATPase with subsequent increase in membrane permeability and ultimately leading to cytotoxic edema. Thus, cerebral cytotoxic edema, whether arising from an ischemic or an epileptogenic cause, can lead to a parallel depression of neuronal metabolism and reduced blood flow to the cerebellar hemisphere contralateral to the supratentorial pathology.
Status epilepticus is a life-threatening condition. The American Epilepsy Society (AES) proposed new guidelines for its treatment in 2016 [8,9]. The guidelines outline a time dependent four phase treatment process. The stabilization phase consists of assessment, monitoring and first aid for seizures. In the initial therapy phase, when it is determined that intervention is required; benzodiazepines are the treatment of choice. The second-line treatment options include intravenous fosphenytoin, valproic acid and levetiracetam. If these medications are unavailable, then intravenous phenobarbital may be given. In the third therapy phase, there is no clear evidence to guide therapy. The second-line therapy may be repeated or an anesthetic dose of thiopental, midazolam, pentobarbital or propofol may be given.
While seizure edema is not an uncommon diagnosis in a busy clinical practice, the presence of associated CCD is exceedingly rare. Nonetheless, it is important for the radiologist to become aware of this interesting association, in order to establish a prompt diagnosis and positively impact patient management.

![]()

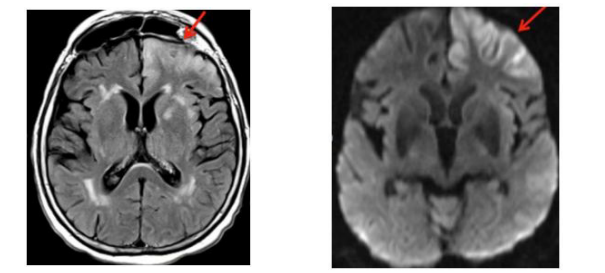 |
| Figure 1: : Seizure related changes in the cortex (a) Axial FLAIR sequences of the brain demonstrates abnormal signal involving the left frontal lobe involving the cingulate gyrus, the inferior and middle frontal gyri, and extending laterally to the frontal operculum with associated sulcal effacement; (b) Diffusion weighted images demonstrating similar areas with restricted diffusion |
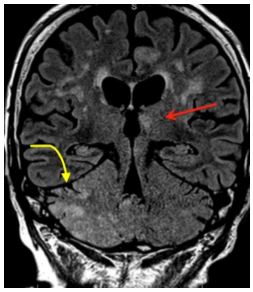 |
| Figure 2: Seizure related changes in the deep grey nuclei. Coronal FLAIR sequences of the brain demonstrate abnormal signal within the left anteromedial thalamus and portions of the striatum (straight arrow). No associated restricted diffusion was demonstrated. Extensive signal abnormality is seen in the right cerebellar hemisphere, compatible with CCD (curved arrow) |
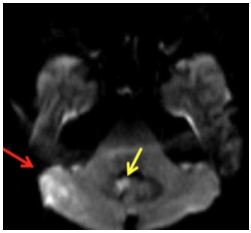 |
| Figure 3: Crossed cerebellar diaschisis. Diffusion weighted images demonstrate restricted diffusion along the posterior aspect of the right cerebellum (red arrow), and tonsils (yellow arrow) |




































