Open Access
Research Article
Max Screen
ISSN: 2456-5504
Copyright: © 2019 D’Amato D. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Congenital anorchia is an uncommon clinical condition. Etiology and pathogenetic mechanisms are often unknown. Although some patients with anorchia present with ambiguous external genitalia or micropenis, most have a normal phenotype.
XY Disorders of Sex Development classifications are numerous and success rate in establishing a precise diagnosis is far lower than in XX karyotype
We report the case of a young man, with 46 XY karyotype showing various uro-genital abnormalities.
A definitive diagnosis was not established due to the complex clinical presentation. Ultrasonography and Magnetic Resonance Imaging techniques were useful tools in the definition of uro-genital anomalies and gonadal development in this complex scenario.
Keywords: Anorchia; Cryptorchidism; Urogenital Anomalies; DSD; MRI
List of abbreviations: MRI: Magnetic Resonance Imaging; US: Ultrasonography; DSD: Disorders of Sex Development, FSH: FollicleStimulating Hormone; HCG: Human Chorionic Gonadotropin;LH: Luteinizing Hormone; AMH Antimüllerian Hormone; LHRH LHReleasing Hormone; SD: Standard Deviation
The disorders of sexual differentiation constitute a challenging area for both diagnostic and therapeutic impact. When presenting late in an adult the therapeutic as well as diagnostic issues may be different and difficult. Bilateral anorchia is rare. Adult disorders of sexual differentiation (DSD) are on the rise due to the diagnostic advances in laboratory and imaging sciences. Thus, presenting with not only the increase in number of cases but also certain diagnostic as well as therapeutic issues. The causes of non-palpable gonads (testes) in a male child are anorchia, inguinal testes, and intra-abdominal testes. Absence of testes in a 46, XY individual with a male phenotype (TRS) or “vanishing testis syndrome” occurs when because of the subsequent atrophy and disappearance in fetal life of an initially present and identified normal testis. The familial occurrence of anorchia [1,2] and its association with other anomalies [3] suggests a genetic origin, but the genetic cause remains unknown. However in a certain number of cases in the early stages of development this condition correlates with a vascular hypo-influx and a testicular torsion [4].
A 27-year-old man complaining impotence and infertility came to our Institution for hormonal, imaging and chromosomal assessments. His past medical history was unknown due to language barriers.
Physical examination showed micropenis with dorsal erect penile length being lower than 2 standard deviation (SD) smaller than the mean human penis size for age and non-palpable testicles. Scrotum was absent.
Furthermore phenotypic appearance of the patient did not show other physical anomalies that could suggest a syndromic disorder.
He performed some blood tests that showed serum basal level of testosterone < 0.5 nmol/L (normal values 11-59 nmol/L) and that did not change after administration of human chorionic gonadotropin (hCG). Luteinizing hormone (LH) and follicle-stimulating hormone (FSH) circulating levels were above normal range and moreover administration of LH- releasing hormone (LHRH) induced and prolonged increase in this hormone levels. Serum antimüllerian hormone (AMH) and inhibin B levels were undetectable.
Ultrasonography on the pelvis was carried out showing absence of prostate gland and seminal vesicles. No testicles were detected in both inguinal canals.
Therefore; the patient performed pelvic Magnetic Resonance Imaging (MRI) examination with a 1.5-T scanner” (Intera, Philips, The Netherlands) using T2 weighted sequences in axial, coronal and sagittal planes
MRI confirmed absent scrotum, testicles, epididymis, prostate gland and seminal vesicles. Furthermore, MRI showed absent corpus spongiosum with normal corpus cavernosum”. Bladder and urethra were normally detectable.
No images compatible with undescended testicles were evident (Figures 1,2 and 3) Subsequently the patient underwent karyotype analysis showing an XY profile.
The laboratory tests and the diagnostic investigations to which the patient has been subjected have led us to formulate the diagnostic suspicion of a condition falling within the spectrum of sexual disorders and in this case bilateral congenital anorchia.
Unilateral congenital anorchia affects one in 5,000 males and bilateral congenital anorchia affects one in 20,000 males [5-8].
The actual incidence may be higher, because one fifth of cryptorchid patients at age 12 months or older are found to have no palpable gonad [8]. Although some patients with anorchia present with ambiguous external genitalia [9] or micropenis [10], most have a normal phenotype.
Disorders of sex development (DSD) of XY karyotype are numerous, but paradoxically the success rate in establishing a precise diagnosis is far lower than in XX DSD.
SRY mutations are the most common cause of complete gonadal dysgenesis (Swyer syndrome), but a definite mutation of the gene can been founded in the 10-15% of cases. This observation suggested that a multitude of other genes must be involved in testicles determination [3-8,11,12]. Moreover some Authors observed that some disorders may be caused by the effects of environmental chemicals on the developing male reproductive tract [12-14]. Ultrasonography is the modality of choice in evaluation of orthotopic testicles. However ultrasound is not sensitive when looking for intra-abdominal testicles (ultrasound has sensitivity as high as 95- 97% when locating an inguinal testicle). In this case MRI may be useful in identifying an intra-abdominal testis [15].
Various case reports with different characteristics and combinations of urogenital abnormalities have been described in literature [2,3,16-18].
We report about young man who complained impotence and infertility, who showed a combination of various uro-genital abnormalities and no other anomalies that could include them in a syndromic disorder. In addition patient’s karyotype appeared to be 46 XY.
MRI is the best imaging modality for diagnosing genital tract developmental anomalies in male as the anatomic delineation is precise, because of its multiplanar capability, superior soft-tissue contrast and lack of ionizing radiation [19].
Diagnostic imaging is usually not necessary for determining the total absence of testicles and ductus deferens because diagnosis can be made by clinical examination, although absence can be confirmed by MRI that is fundamental to exclude any testicles in pelvis or abdomen [20]. Imaging plays an important role in evaluating the internal organs and urogenital anatomy in the disorders of sexual differentiation. Ultrasonography (US) and magnetic resonance imaging (MRI) are used for diagnosing a non-palpable testis, because they are basically non-invasive, do not involve radiation load, and have a detection rate that is similar to other diagnostic methods. Ultrasonography remains the primary modality for evaluation of the internal reproductive organs, while MR imaging may serve as a problem solving modality for clarifying the internal anatomy and searching for internal gonads [21-29].
T1 and T2 weighted MR imaging sequences with their multiplanar capability superior tissue characteristics can provide detailed anatomic information. MR imaging is more sensitive than US in the evaluation of the gonads [28].
MR imaging and US are considered equally sensitive in the evaluation of intrapelvic structures. However, MR imaging is more sensitive than US in detecting the gonads [28].
MRI is more sensitive than US, and does not entail either ionizing radiation or intravascular contrast medium. MRI is capable of producing multiplanar images and has the potential for tissue characterization. In addition, it allows global, multiplanar depiction of the anatomy of the retroperitoneum and inguinal region in a single study with the coronal plane and the axial plane. Fritzsche et al. first reported successful MRI localization before surgery for undescended testis in 15 (93.7%) of 16 non-palpable testes in 12 patients, in which there was one false negative finding. Kier et al. located five (62%) of eight non-palpable testes by using MRI and obtained three false- negative results. Miyano et al. located nine (81.8%) of 11 non-palpable testes by using MRI and obtained two false negative findings, which were confirmed by surgery [23-25].
Several pathogenetic factors are involved and in order to achieve a precise diagnosis a multidisciplinary endocrinological, urological, radiological and genetic approach is often needed. The clinical case we reported is part of primary male hypogonadism, where clinical and laboratory aspects can be traced back to congenital absence of gonads, prostate gland, seminal vesicles, epididymis, and spermatic cords.
Primary hypogonadism can be treated with several strategies in pre-puberal phase, however, in the case we examined, the diagnosis took place in post-puberty and the most appropriate approach is hormone replacement therapy [30].
It is very important to carry out this kind of therapeutic approach because chronic androgen deficiency can result in osteoporosis, muscle weakness, anemia, increase in visceral fat mass, depression as well as infertility. Treatment is also important for enhancing insulin sensitivity, improving lipid profile and consequently reducing cardiovascular risk [31-33].
Therefore, in relation to the impact of male hormones on different target tissues, it is essential to perform hematochemical blood tests such as hemoglobin, hematocrit, serum iron, total iron-binding capacity (TIBC), and/or transferrin tests, vitamin D levels, and instrumental examinations such as Bone Densitometry
It is the general consensus to treat men with age-related hypogonadism only when clinical symptoms are present [34-36].
For our Patient the most appropriate type of formulation is decided by the endocrinologist specialist.

![]()

 |
| Absence of spongy body of urethra, with Absence of corpus spongiosum, with normal corpus
cavernousum. MRI confirmed the absent scrotum sac, testicles, epididymis and related spermatic cords.
Normal representation of bladder- urethral junction. Normal representation of remaining pelvic organs. Figure 1: Sagittal T2-weighted image of pelvic district |
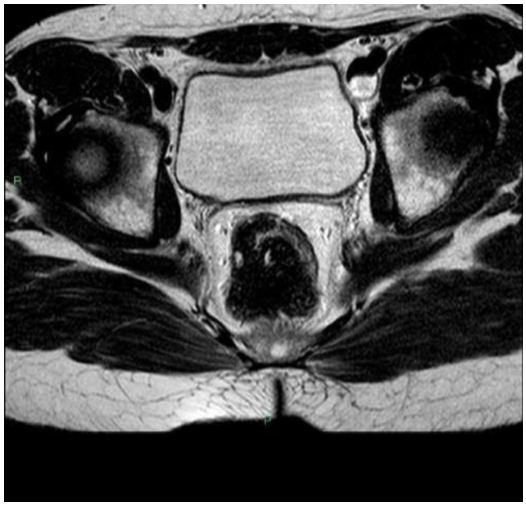 |
| No images compatible with undescended testicles are evident. Figure 2: Figure 2: Axial T2- weighted image of the pelvic district |
 |
| Prostate gland and seminal vesicles are not evident. Figure 3: Coronal T2 weighted image of pelvic district |




































