Open Access
Research Article
Max Screen
ISSN: 2456-5504
Copyright: © 2018 Chau SF. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Aim and Objectives:Giant cell arteritis (GCA) requires prompt diagnosis as clinical indicators of GCA are non-specific. Temporal artery biopsy (TAB) can be inconclusive and difficult to arrange timely. MR imaging is accurate for showing vessel thickening. However, availability of MRI remains an issue in many radiology departments. Whilst multi-centre trial (TABUL trial) is evaluating the role of ultrasound, a local study has been carried out independently of the TABUL trial to investigate the diagnostic performance of ultrasound for GCA, namely by correlating ultrasound findings and diagnostic outcomes in a selective high-risk group of patients. Study was started prior to initial results from the TABUL trial were published.
Methods and Materials:Prospective study was carried out over 2 years including 14 patients referred by rheumatologists with presumed new diagnoses of GCA. Symptoms included headache, visual loss, jaw claudication and raised ESR. Ultrasound of both temporal arteries was performed. Abnormal findings included mural thickening (>1mm), halo sign around colour Doppler in lumen and specific discomfort on sono-palpation of vessel on the affected side. All clinical treatments were reviewed.
Results:10/14 patients demonstrated abnormal scans with segmental mural thickening/halo sign or positive sono-palpation along the temporal artery. 9 patients turned out to have GCA and were subsequently managed as such (sensitivity = 90%).
4/14 patients demonstrated normal scans, 3 of whom were not clinically treated as GCA (specificity = 75%)
Good correlation was present between vessel wall thickening and focal tenderness on vessel sono-palpation
Median number of days from referral to scan was 0 (same day) for inpatients (range 0-1), outpatients 4 days (range 0-27).
Conclusion:Temporal artery ultrasound allows non-invasive, cost-effective and prompt assessment of GCA and demonstrated good diagnostic accuracy in this subset of selected group of patients. This study will be of particular value in environment such as UK National Health Service where resources are limited with no financial incentive for over-investigating patients.
Keywords: Arteries; Inflammation; Connective tissue disorders; Ultrasound-Colour Doppler; Vascular
List of Abbreviations:ACR: American College of Rheumatology; CDA: Clinical Document Architecture; CRIS: Clinical Radiology Information System; EULAR: European League against Rheumatism; GCA: Giant Cell Arteritis; MRI: Magnetic Resonance Imaging; PMR: Polymyalgia Rheumatica; TAB: Temporary Artery Biopsy; TABUL: Temporal Artery Biopsy vs Ultrasound; US: Ultrasound
Giant cell arteritis (GCA) typically affects the elderly population (aged ≥50) with female preponderance (incidence of 3.5 per 100 000 per year). The clinical symptoms can be categorised into those caused by cranial vascular involvement, those due to arteritis of large vessels, systemic inflammatory signs, and polymyalgia rheumatica (Table 1 and Figure 1). It requires prompt diagnosis in order to avoid complications such as blindness [1-3]. The characteristic symptoms are emphasized in the 2012 classification criteria of the European (EULAR) and American (ACR) rheumatology societies (Table 2) [4]. However, clinical indicators of GCA are non-specific, and temporal artery biopsy (TAB) is not entirely sensitive and often difficult to arrange timely. Serious risks of biopsy include injury to the branches of the auriculotemporal or facial nerve, as well as bleeding and wound infection.
Patients with often non-specific symptoms are started on high dose steroids which are often continued for a significant period of time. There are often logistical problems with performing a surgical temporal artery biopsy which can often be inconclusive. The dilemma for the clinician is to assess the level of risk to the patient. There are significant ischaemic related complications from developing GCA (Table 3 and Figure 2), as well as significant complications from high dose steroids (Table 4) [6,7]. The clinician needs a simple test to triage the patient’s clinical treatment of course.
A previous study on MRI in GCA has already demonstrated good diagnostic value [8], with a sensitivity of 80.6% and a specificity of 97.0% based on evaluation of the mural inflammatory sign (Figure 3). However, availability of MRI remains an issue in many radiology departments.
The TABUL Trial is an ongoing UK multi-centre randomised prospective trial since 2010 which evaluates the diagnostic accuracy of ultrasound in GCA as an alternative to TAB [9]. Early results from 2015 have been promising in showing a significant proportion of new GCA cases (46%) have demonstrated the “halo” sign (Figure 4), corresponding to oedema of the intimal layer of the artery seen histologically (Figure 5). This correlated significantly with both ischaemic symptoms and abnormal physical examination. The likelihood of finding a halo diminishes with duration of steroid therapy [10].
Our study aimed to assess the diagnostic performance of ultrasound for GCA by correlating ultrasound findings and subsequent diagnostic outcomes in a sub-selected high-risk group of patients in a district general hospital. The study was independent of the TABUL trial and started long before the results of TABUL trial were published.
A prospective study was carried out over 2 years (Oct 2013 - Sept 2015) including 14 patients referred by rheumatologists with presumed new diagnoses of GCA. Symptoms included headache, visual loss, jaw claudication and raised ESR. Ultrasound of both temporal arteries was performed using GE Logiq E9 machine and 18 MHz hockey stick probe.
An abnormal scan was classed as showing:
• Mural thickening >1mm or vessel diameter >2.5mm
• Halo sign around colour Doppler in lumen (Figure 4)
• Discomfort on sono-palpation of the vessel on the affected side
The decision to use mural thickness > 1mm or vessel diameter (>2.5mm) as diagnostic criteria was based on results from previous MR imaging study [8], which showed in patients with GCA the mean wall thickness increased significantly from 0.39mm (±0.18mm) to 0.74mm (±0.32mm; P < 0.001), and the lumen diameter decreased significantly from 0.84mm (±0.29mm) to 0.65mm (±0.38mm; P < 0.05). The minimum increase in mural thickness that could be reliably detected on ultrasound was 1mm, based on our experience.
Each case was followed up for outcomes with retrospective review of CRIS and CDA (Clinical Document Architecture) system. The time from request to scan was also measured. The patient was asked or medical records examined to see whether steroids were being taken at the time of the ultrasound scan.
Of the 14 patients referred, 10 demonstrated abnormal scans:
• 8/10 scans showed segmental mural thickening or halo sign
• 9/10 scans demonstrated focal discomfort on sono-palpation along the temporal artery.
• 9/10 patients were subsequently treated as GCA with high dose steroids for appropriate time ( sensitivity = 90%).
• 1/10 patient had symptoms and raised ESR because of infection.
4 patients demonstrated normal scans:
• 3/4 cases were not treated as GCA ( specificity = 75%).
• 1/4 cases was for pre-biopsy surface marking of the temporal artery that was not clinically palpable. This patient had relapsing symptoms and was started on a repeat regime of high dose steroids for over two weeks prior to temporal artery biopsy, which was subsequently proved as GCA on histology.
The incidence of halo sign and vessel wall thickening was 8/14 = 57%. One case of bilateral temporal artery halos was identified.
The median number of days from referral to scan was 0 (i.e. same day) for inpatients (range 0 - 1) and 4 days for outpatients (range0 - 27).
Temporal artery ultrasound proves to be a useful test for diagnosing GCA with good sensitivity and specificity. Diagnosis using ultrasound was true-positive in 9 out of 10 patients and true-negative in 3 out of 4 patients. The only false-negative case was for pre-operative marking before elective surgical temporal artery biopsy, and this is possibly down to diminished likelihood of eliciting positive ultrasound findings after the prolonged steroid treatment. We recognise that whilst US investigation is useful in detecting GCA in presence of pathological findings, further examinations are probably required in true negative patients where US imaging is normal.
This study demonstrated a good correlation between vessel wall thickness and focal tenderness on vessel sono-palpation. Vessel wall thickness of > 1mm, vessel diameter of at least 2.5mm, the “halo” sign and symptomatic sono-palpation along the line of the temporal artery, should all be regarded as diagnostic of a positive scan.
Since the likelihood of finding halo sign or significant vessel wall thickening is significantly less after 5 days of steroid therapy (as suggested by TABUL Trial) [10], scan should be performed as soon as possible, ideally within a few days of treatment initiation. The timing of the scan is also important as clinicians have to balance the patient’s level of risk from developing GCA related complications such as blindness and stroke (Table 3) against the side effects of steroids (Table 4), often based on clinical grounds initially. Promptly arranged ultrasound scan will help reach diagnosis and thus minimise those risks. Ultimately, risk from surgical TAB might even be avoided if both ultrasound findings and clinical criteria (as proposed by the EULAR-ACR) are highly suggestive of GCA. This is recognising the fact that even negative TAB findings cannot exclude GCA due to skip lesions [11].
Temporal artery ultrasound allows non-invasive, cost-effective and prompt assessment of GCA and demonstrated good diagnostic accuracy in this sub-selected group of patients. The timing and outcome of the scan will allow the clinician to assess and balance the patient’s level of risk from developing GCA related complications against the side effects of steroids.
It is important to note that this study was done within the capacity of the National Health Service of UK, where resources are limited with no financial incentive for over-investigating patients. In order to effectively triage this difficult-to-manage group of patients and avoid over-investigation therefore, this study will be of value.
The authors would like to thank Ness T, Bley TA, Schmidt WA, et al for use of some of their images and illustrations in the article.

![]()

 |
| Giant cell arteritis (GCA) causes inflammation of certain arteries, especially those near the temples.
Reference: Mayo Foundation for medical education and research Figure 1: Inflamed dilated superficial temporal artery in a patient with GCA |
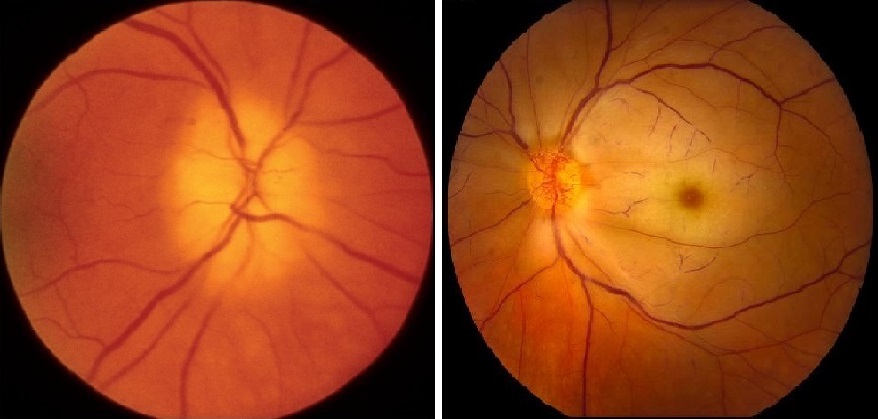 |
| Figure 2: Fundoscopy showing eye complications of GCA (A) Anterior ischaemic optic neuropathy (AION). Optic disc is swollen [5]; (B) Central artery occlusion Reference: Wills Eye Hospital Health Library |
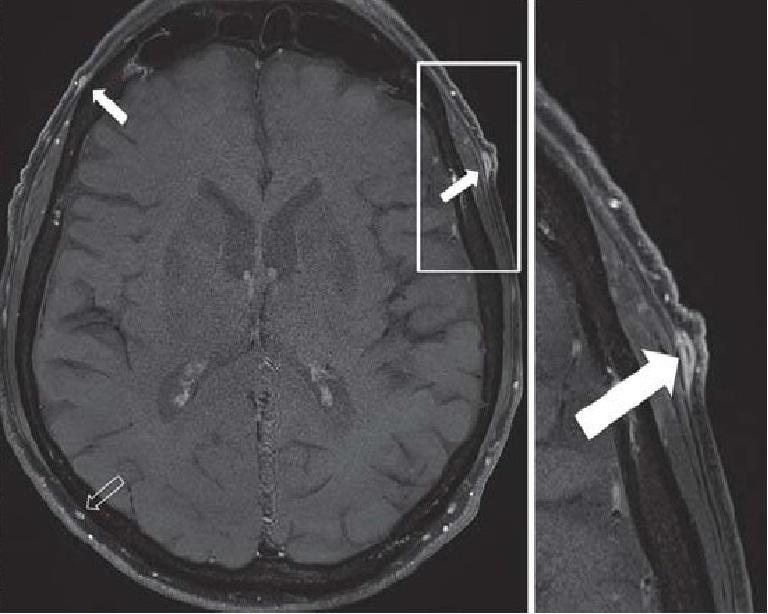 |
| The frontal branch of the superficial temporal artery demonstrates signs of wall inflammation (mural thickening,
uptake of contrast agent). The right superficial occipital artery similarly demonstrates inflammatory changes Figure 3: High-resolution 3T MRI of the superficial cranial arteries in a patient with GCA [1] |
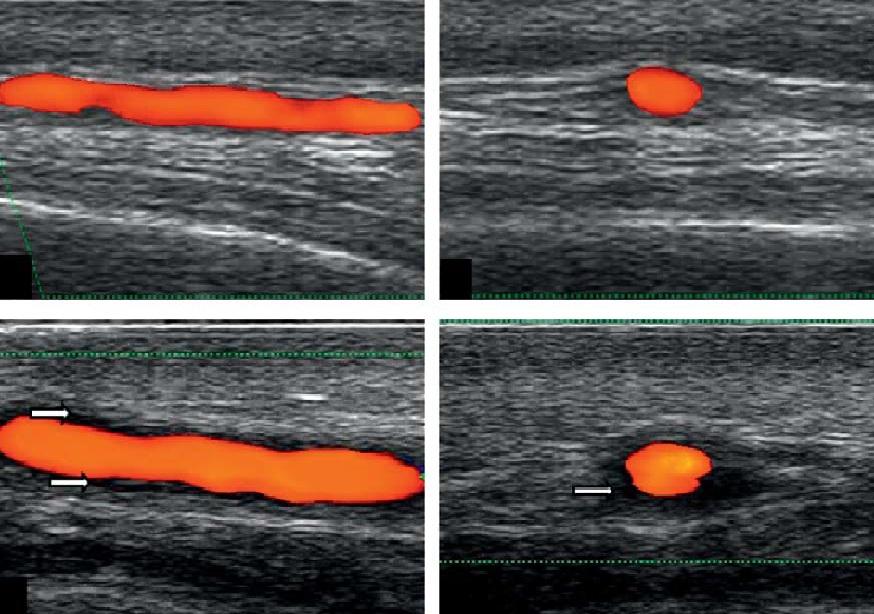 |
| Figure 4: Colour-Doppler ultrasound of the temporal artery (A) and (B) are normal longitudinal & transverse views; (C) and (D) show hypoechoeic “halo” in keeping with mural thickening, in longitudinal and transverse views [1] |
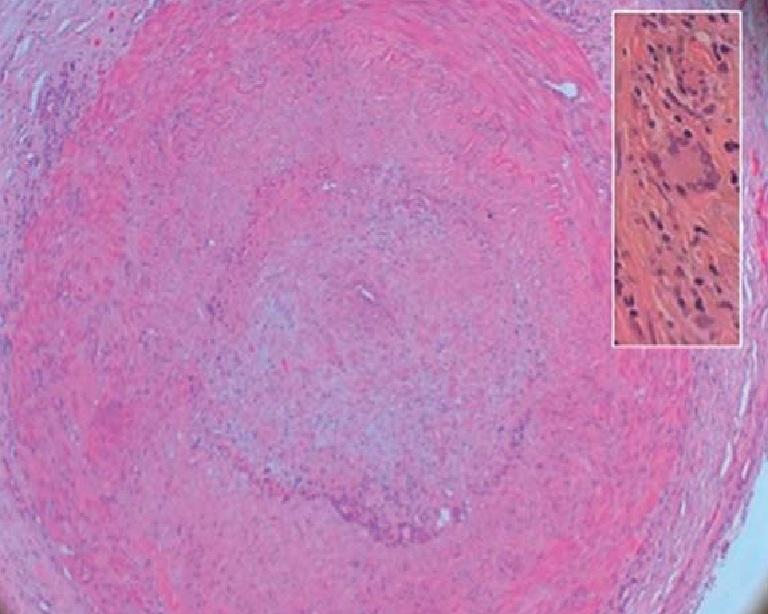 |
| Intimal oedema, cellular infiltration and fragmented internal elastic membrane found in inflamed temporal artery; box:
at the transition between intima and muscularis media in a temporal artery in a case of GCA Figure 5: Histologic findings of inflamed temporal artery [1] |
Category |
Symptoms |
Symptoms due to cranial vessels involvement |
Headache |
Symptoms due to great vessels involvement (aorta and branches of aorta) |
Claudication of extremities |
Symptoms due to systemic inflammation |
Fever, night sweats, weight loss |
Polymyalgia Rheumatica (PMR) |
Proximal myalgia of major trunk muscles (neck, shoulder, pelvic girdles) |
*For GCA, 3 criteria for the classification of GCA must be filled. Classification as PMR requires 4 points [4]. |
Eye manifestations in giant cell arteritis |
|
Some complications from high dose steroids |
|




































