Open Access
Research Article
Max Screen
ISSN: 2574-5980
Copyright: © 2023 KV Surya Teja. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
In the pre-anesthesia era, the anguish of planned surgical maneuver was dreadful and the experience of actual procedure “utterly speechless torture”. Although, the concept of pain relief and even total insensibility was not unfamiliar to medical profession, some of the “Big Giants in Medicine” believed “knife and pain as inseparable” and the efforts to relieve or prevent pain “in vain”. In such a situation the anesthesia,one of the greatest boons of science for mankind, “burst like a revolution on medical profession”. Despite hostility from religious sect, professional colleagues and civil societies the pioneers in discovery of anesthesia stood firm, unshaken by the negative criticism. Although the fate of the active contestant of “Ether Controversy” was mournful,their untiring and dedicated struggle to relieve the sufferings of mankind can never be underscored. Renowned Arab surgeon Ibn al Quff (1232-1286 AD) was the first to suggest anesthesia as independent speciality. However, it took almost 700 years for his dream to come true.
Background:Large numbers of nations are associated with utilization of anti-toxins regardless of remedy (OTC medications). This DDD/ATC value contributes to improved antibiotic use quality. The principal objective is to direct improvement of sane medication use of strategies and to give a standard technique for information for future evaluation.
Aim and Objective:This study aims to examine the drug use and ATC/DDD evaluation of antibiotics in specific departments of a tertiary care hospital in a retrospective fashion. To sort the case reports of patients in light of socioeconomics, we likewise recognized the most regularly involved anti-infection agents in various sicknesses and divisions, alongside examining drug use designs in view of WHO rules, assessing therapy diagrams in view of course of organization, and furthermore researching the significance of units of estimation in measuring anti-toxins utilizing ATC/DDD methodology.
Methods:During our ward participation of inpatient departments from September 2017 to December 2019, data would be reviewed within six months from treatment charts, prescriptions, and case sheets of in-patients admitted to specific departments like General Medicine, General Surgery, and Orthopaedics. It was a cross-sectional, retrospective, and observational study on inpatients at Government General Hospital, Kadapa.
Results:In this review, a sum of 900 subjects treated with anti-toxins were incorporated. There were 499 female subjects (55.5%) and 401 male subjects (44.5%). The average number of drugs prescribed per encounter (2%), the percentage of drugs with generic names (96%), the percentage of drugs prescribed from the essential drug list (100%), and the percentage of drugs prescribed as antibiotics (100%) were all found in this study
Conclusion:In this study, antibiotics were used for six months in a tertiary care hospital. Both the percentage of antibiotic use and the DDD/100 bed-days were used to calculate antibiotic use. In the study, penicillin, a broad-spectrum cephalosporin, was used more. The fact that generic prescribing is declining demonstrates the need to examine and enhance all of these parameters in order to provide the patient with quality and rational treatment.
Keywords: Antibiotics; Atc/Ddd Value; Drug Utilisation Evaluation (Due); Rational Drug Use; Irrational Drug Use
Antibiotics are used to treat only bacterial infections. Usually, an antibiotic is a substance that inhibits and kills the growth of other microorganisms. Many countries are involved in the usage of antibiotics and they are the largest single group of drugs purchased for the development of antibiotics [1]. The greater the use of antibiotics, whether appropriate or not, exerts selective pressure by reducing the reproductive success of microorganisms and, here, by speeding up the development of antimicrobial resistance (AMR) [2]. Drug utilisation is defined by the WHO as the “marketing, distribution, prescription, and use of drug in society, with special emphasis on the resulting medical, social, and economic consequences” [3]. Studies on drug usage evaluation serve as a tool to assess the quality of therapeutic care and evaluate drug usage and play an important role in improving drug dispensing policies in tertiary care hospitals at each and every level to promote the rational use of antibiotics [4]. The drug usage pattern is being studied to analyse the present scenario and the development of drug usage at various levels of the healthcare system [5].
The Anatomical Therapeutic Chemical (ATC) code is a tool to express drug utilisation research in order to improve the quality of drug use. DDD is appropriate for drugs that have already been provided with an ATC code. These parameters are useful for evaluating drug utilization at every level of the healthcare system [6]. To assess the units of measurement used to quantify antibiotic use and discussions about the interpretation of these units are rarely presented in the scientific literature.
DDDper1000persons per day = N×M×Q×1000/DDD×P×T
Where
The ultimate goal is to guide the development of rational-use drug policies and to provide a standard method of data for future assessment [9]. Rational drug use is a quality healthcare service, particularly in the use of antibiotics and also its usage that is cost-effective with increasing drug toxicity, clinical therapeutic effects, and minimising the occurrence of resistance [10]. Irrational use of medicine is the use of too many medicines per patient (polypharmacy), inappropriate use of antibiotics, inadequate dosage for non-bacterial infections, failure to prescribe under clinical guidelines, inappropriate self-medication, and also overuse of prescribed medicines [11]. Hence, the current study was conducted to assess the Drug utilization and ATC/DDD evaluation of antibiotics in specific departments of a tertiary care hospital: a retrospective study in Government General Hospital (GGH) – Kadapa, Andhra Pradesh [12].
The purpose of this study is to conduct a retrospective investigation into the drug utilisation and ATC/DDD evaluation of antibiotics in specific departments of a tertiary care hospital and to evaluate the drug utilisation and ATC/DDD evaluation of antibiotics in specific departments of a tertiary care hospital.
Data was be collected from treatment charts, prescriptions, and case sheets of the in-patients who are admitted to specific departments such as General Medicine, General Surgery, and Orthopaedics during our ward participation of inpatients departments from September 2017–December 2019.
It was a retrospective, observational, cross-sectional type of study was conducted on the in-patients at Government General Hospital, Kadapa.
The total sample size was about 900 patients.
1. The study included if the subject satisfies the following criteria:
2. Patients admitted to the in-patient unit, regardless of gende
3. Patients who had undergone antibiotic treatment between the ages of 20 and 80
4. Patients admitted in the specific department such as General Medicine, General surgery and Orthopaedics.
5. Antibiotics available in the G.G.H Essential Drug List
6. Antibiotics are prescribed in different drug dosage forms.
All patients who are prescribed at least one antibiotic and are admitted to specific departments such as General Medicine, General Surgery, and Orthopaedics
Exclusion Criteria:The study excluded the following people:
1. Patients who are allergic to antibiotics
2. Paediatric population
All the data of recruited subjects was entered into a Microsoft excel spreadsheet then Descriptive statistics like mean, standard deviation was used to assess the different demographic parameters. We assigned an ATC code to the antibiotic use and calculation of DDD/100 bed-days themost commonly used antimicrobials were classified using the ATC Classification system, and drug utilisation was measured as DDD/100 bed-days. In the ATC Classification system, drugs are divided into different groups according to the organ or system on which they act and their chemical, pharmacological, and therapeutic properties.
A total of 900 samples were collected from December 2020 to May 2021 in a period of 6 months, among them 300 samples were collected from 2017 medical record department,300 samples were collected from 2018 medical record department and 300 samples were collected from 2019 medical record department.
Most commonly used antibiotics in general medicine for common diseases are pneumonia, pancreatitis, thrombocytopenia, malaria, CKD, tuberculosis, PUD, COPD, liver cirrhosis, epilepsy, jaundice, bronchial asthma, hepatomegaly, ALD, PID, Takayasis arteritis, endocarditis, cad,oedema, typhoid fever, uti, parkinsons, gastritis, stroke, jaundice, gastroenteritis, seizures, asthma, anaemia, cholecystitis, hypoalbuminemia. The most commonly used antibiotics are ceftriaxone, amoxicillin with clavulanic acid, ampicillin, piperacillin with tazobactam, cefperazone with salbactam, cefotaxime, cefixime, amikacin, streptomycin, gentamicin, doxycycline, azithromycin, ciprofloxacin, levofloxacin, ofloxacin, norfloxacin, gatifloxacin, metronidazole, cotrimoxazole (sulphamethoxazole + trimethoprim), nitrofurantoin. (Shown in table 4)
Most commonly used antibiotics in general surgery for common diseases are appendectomy, hernia, IBD, varicose veins, trauma ulcer, necrosing fasciitis, synovitis, pancreatitis, cellulitis. The most commonly used antibiotics are ceftriaxone, gentamicin, amoxicillin with clavulanic acid, ampicillin, piperacillin with tazobactam. (Shown in table 5).
Most commonly used antibiotics in orthopaedics for common diseases are rheumatoid arthritis, osteoarthritis, arthralgia, low backpain, hip fracture, fractures, tennis elbow. The most commonly used antibiotics are ceftriaxone, gentamicin, amoxicillin with clavulanic acid, doxycycline, piperacillin with tazobactam, ciprofloxacin. (Shown in table 6).
The WHO assigned DDD was mentioned in the table number. Our study results were below the standard DDD, which indicates rational prescribing. All the antibiotics used in In-patient were found to be rational. The observed value of commonly used antibiotics in General Medicine were ceftriaxone (0.11), Amoxicillin and potassium clavulanate/ clavulanic acid(0.12), Ampicillin (0.06), Piperacillin with tazobactam (0.032),Cefperazone with salbactam (0.005), Cefotaxime (0), Cefixime (0.12), Amikacin (0.001), Streptomycin (0.003), Gentamicin (0.02), Doxycycline (0.426), Azithromycin (0.426), Ciprofloxacin (0.006), Levofloxacin (0.095), Ofloxacin (0.18), Norfloxacin (0.002), Metronidazole (0.001), Cotrimoxazole (0.16), Nitrofurantoin (0.007). (Shown in table 7).
The WHO assigned DDD was mentioned in the table number. Our study results were below the standard DDD, which indicates rational prescribing. All the antibiotics used in In-patient were found to be rational. The observed value of commonly used antibiotics in General Surgery were Ceftriaxone (0.065), Amoxicillin with potassium clavulanate/ clavulanic acid (0.32), Piperacillin with tazobactam (0.005), Ampicillin (0.005), Gentamicin (0.081), Ciprofloxacin (0.020). (Shown in table 8)
The WHO assigned DDD was mentioned in the table number. Our study results were below the standard DDD, which indicates rational prescribing. All the antibiotics used in In-patient were found to be rational. The observed value of commonly used antibiotics in Orthopaedics were Ceftriaxone (0.03), Amoxicillin with potassium clavulanate/ clavulanic acid (0.058), Piperacillin with tazobactam (0.0086), Doxycycline (0.58), Gentamicin (0.17), Ciprofloxacin (0.011). In this Moderate usage of antibiotics had more ATC/DDD value of antibiotics. (Shown in table 9).
Our clinical study was conducted on the drug utilisation and ATC/DDD evaluation of antibiotics in specific departments of a tertiary care hospital. It was found that slightly more female patients were admitted to the various departments in the hospital when compared to male patients. Prescribed drugs by generic names would make it easier for the hospital to have control over its regulatory stock and also lower the cost of treatment. Most patients were involved in IV therapy only
In this study, we concluded that, according to WHO standards, every drug must be prescribed with a generic name. to avoid this type of confusion between different classes of drugs with nearly similar brand names while dispensing and also to decrease the cost of therapy which is similar to the study of Kanishk Kala et.al., in 2019 [3]. Some key indicators, such as the number of drugs prescribed under generic names and the number of drugs on the essential medicine list, should always be close and also mentioned depending on the clinical needs of the patients which is similar to the study of Ajaya kumar sahoo et.al., in 2020 [4]. In a majority of the 900 cases, a majority of the drugs were purely prescribed based on their generic names (97.33%) which is similar to Nilay Solanki et.al. in 2019 [5]. In this study, the prescribing frequency of antibiotics per prescription is mostly one (40.33%) or two (26.11%) was Ceftriaxone and Amoxycillin and potassium clavulanate / clavulanic acid were the most commonly prescribed medications in the general medicine, general surgery, and orthopaedics departments respectively were found to be effective for treating infections both empirically and prophylactically. which is similar to R. Suraj et.al., in 2008 [7].
This study reports the use of antibiotics in a tertiary care hospital for six months. Antibiotic usage was calculated in both the percentage of antibiotic use and DDD/100 bed-days. ATC-DDD system which is accepted globally can be used in antibiotic usage studies for better expression and possible cross comparisonacross similar studies. The use of antibiotics usually broad-spectrum cephalosporins, pencillins was high in the study. A high average number of drugs per prescription along with high use of injections was noted. Generic prescribing is less this shows that all these parameters should be checked and improved to provide quality and rational treatment to the patient.
Nil

![]()

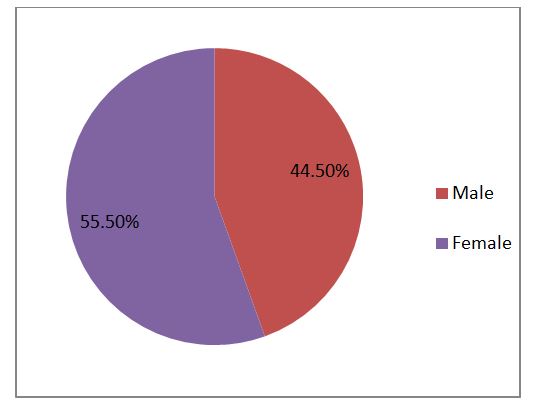 |
| Figure 1: Gender wise Distribution In this study, a total of 900 subjects treated with antibiotics were included. Among them 401 subjects were males (44.5%) and 499 subjects were females (55.5%). (Shown in figure 1) |
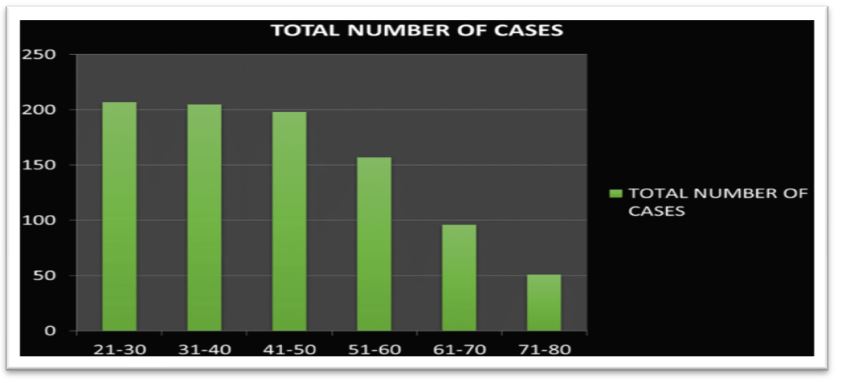 |
| Figure 2: Age group Categorization This study included 900 patients and out of them most of the patients was observed from the age group between 21-30 years (23%), next from the age group 31-40 years (22.9%), next from the age group 41-50 years (19.9%), next from the age group 51-60 years (17.7%), next from the age group 61-70 years (10.7%) and the age group 71-80 years (5.8%) (Shown in figure 2) |
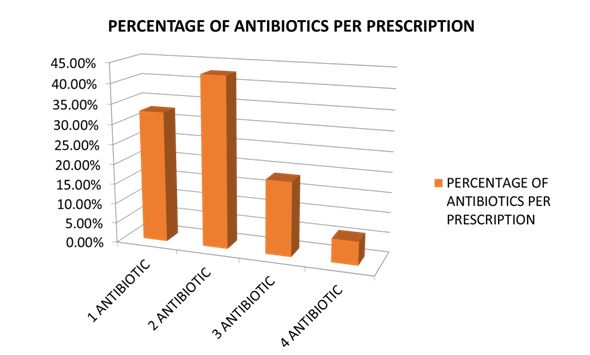 |
| Figure 3: Based on Number of Antibiotics per Prescription In this study, the antibiotics per prescription per patient of 1 antibiotic 295 (32.8%), 2 antibiotics 385 (42.7%), 3 antibiotics are 167 (18.6%) and 4 number of antibiotics per prescription per patient are 53 (5.9%). (Shown in figure 3). |
S. No |
Route of administration |
Total |
Percentage |
1 |
ORAL |
531 |
59 % |
2 |
IV |
807 |
89.7% |
S.No |
Department |
Average length of stay |
1 |
General medicine |
3.5 days |
2 |
Orthopedics |
4 days |
3 |
General surgery |
5 days |
WHO Core Prescribing Indicators |
Value |
The average number of drugs per encounter |
2 |
Percentage encounter prescribed injections |
59 % |
Percentage of drugs with generic names |
96 % |
Percentage of drugs prescribed in the essential drug list |
100 % |
Percentage encounter prescribed antibiotics |
100 % |
Department |
Disease |
Drugs |
General Medicine 300(100%) |
Pneumonia 15(5%) |
Amoxicillin 63(50%) |
Department |
Diseases |
Drugs |
General Surgery 300 (100%) |
Appendectomy 30(10%) |
Ceftriaxone 129(100%) |
Department |
Diseases |
Drugs |
Orthopedics 300 (100%) |
Rheumatoid Arthritis 74(24.6%) |
Ceftriaxone 69(100%) |
S. No |
Antibiotics |
ATC Code |
DDD Value/ 1000 Inhabitants (mg) |
WHO Code (g) |
Ceftriaxone |
J01dd04 |
0.11 |
2 |
|
Amoxicillin With Clavulanic Acid |
J01cr02 |
0.12 |
1.5 |
|
Ampicillin |
J01ca01 |
0.06 |
2 |
|
Piperacillin With Tazobactam |
J01cr05 |
0.0032 |
14 |
|
Cefperazone With Sulbactam |
J01dd62 |
0.005 |
4 |
|
Cefotaxime |
J01dd01 |
0 |
4 |
|
Cefixime |
J01dd08 |
0.12 |
0.4 |
|
Amikacin |
J01gb06 |
0.001 |
1 |
|
Streptomycin |
J01ga01 |
0.003 |
1 |
|
Gentamicin |
J01gb03 |
0.02 |
0.24 |
|
Doxycycline |
J01aa02 |
0.426 |
0.1 |
|
Azithromycin |
J01fa10 |
0.426 |
0.3 |
|
Ciprofloxacin |
J01ma02 |
0.006 |
1 |
|
Levofloxacin |
J01ma12 |
0.095 |
0.24 |
|
Ofloxacin |
J01ma01 |
0.18 |
0.4 |
|
Norfloxacin |
J01ma06 |
0.002 |
0.8 |
|
Metronidazole |
J01xd01 |
0.001 |
1.5 |
|
Cotrimoxazole (Sulphamethoxazole + Trimethoprim) |
J01ee01 |
0.16 |
1.06 |
|
Nitrofurantoin |
J01xe01 |
0.007 |
0.2 |
S. No |
Antibiotics |
Atc Code |
Ddd Value/ 1000 Inhabitants |
Who Ddd Value (G) |
Ceftriaxone |
J01dd04 |
0.065 |
2 |
|
Amoxicillin With Clavulanic Acid |
J01cr02 |
0.32 |
1.5 |
|
Piperacillin With Tazobactam |
J01cr05 |
0.005 |
14 |
|
Ampicillin |
J01ca01 |
0.005 |
2 |
|
Gentamicin |
J01gb03 |
0.081 |
0.24 |
|
Ciprofloxacin |
J01ma02 |
0.020 |
1 |
S. No |
Antibiotics |
ATC Code |
DDD Value/ 1000 inhabitants |
WHO DDD Value (g) |
Ceftriaxone |
J01DD04 |
0.03 |
2 |
|
Amoxicillin With Clavulanic Acid |
J01CR02 |
0.058 |
1.5 |
|
Piperacillin With Tazobactam |
J01CR05 |
0.0086 |
14 |
|
Doxycycline |
J01AA02 |
0.58 |
0.1 |
|
Gentamicin |
J01GB03 |
0.17 |
0.24 |
|
Ciprofloxacin |
J01MA02 |
0.011 |
1 |




































